
The Effect of Comprehensive Feeding Practices and Physical
Activities on the Over-nutritional Status of Preschoolers in the
Working Area of Juanda Community Health Center Samarinda
Debora Injilia Hartati, Reny Noviasty and Rahmi Susanti
Department of Public Health Mulawarman, Samarinda, Indonesia
Keywords: Physical Activity, Overweight, Comprehensive Feeding Practices, Preschool.
Abstract: The prevalence of obesity in children under five based on the latest Riskesdas (2018) is 8.0%. This is still a
nutritional problem in Indonesia¸ although it’s has shown a decrease case. Because it’s causing other health
problems. This study aimed to determine the effect of comprehensive feeding practices and physical activity
on over nutritional status in preschool children at the working area of Puskesmas Juanda. The design of the
study was a case control 1:2 with a total sample 36 IRT. Primary data collection used the CFPQ and Pre-PAQ,
as well as secondary data through the latest posyandu weighing records. Data analysis used Chi Square test
and Odds Ratio with a significance value of 0.05. The results showed that there was an effect of
comprehensive feeding practices (p = 0.001; OR=26,714) and physical activity (p = 0.000; OR=33) on the
over-nutrition status of preschool children (3-5 years) in the working area of Juanda Community Health
Center Samarinda. It’s advisable for mothers to pay more attention to the needs of the child's nutritional needs
when feeding, and to support the child more actively by bringing the child to an open space area regularly (at
least 180 minutes a day for children to move actively).
1 INTRODUCTION
Global data in 2018 shows that the number of under-
fives who are over-nutrition is estimated at 5.9% (40
million) children, almost half of whom live in Asia
and a quarter live in Africa. Since 2000-2018 cases of
overnutrition in children under five in all countries
have increased by 10 million cases. (UNICEF, WHO
and The World Bank, 2019). In 2019 there were 38
million children under five who were overweight and
obese (WHO, 2020).
Based on the latest trends, the number of children
under five who are overnutrition is expected to
increase (from 40 million children) to 43 million in
2025. Therefore, WHO sees that the problem of
obesity in children under five is one of their attention
focuses, because besides being important for the
welfare of children, nutrition is also needed in
achieving sustainable development goals. So that
WHO sets obesity as one of the SDGs indicators and
sets it as a global target to stop the increase in obesity
by 2025 (UNICEF, 2019).
Indonesia's national data, according to Riskesdas
in the last years 2018 (8,0%), has actually alredy
shown a declining trend of over nutrition and obesity
(BB/TB > 2 SD) (Kemenkes RI, 2019). However, it
is still a nutritional problem in Indonesia because it is
a contributor to the incidence of global obesity which
must continue to be suppressed, because it is at risk
of causing new problems, namely health problems,
especially the increase in the incidence of PTM that
arises faster than age in general (Kemenkes RI, 2020).
Indonesian national data shows that there are still
12 provinces with prevalence of overweight and
obesity (Z score according to BB/TB > 2 SD) above
the national prevalence in 2018, including East
Kalimantan which is in the 6th highest rank after the
national prevalence, with a percentage by 9.4%
(Kemenkes RI, 2019). Then seen from DKP Kaltim
data obtained through PSG in the last 3 years for over
nutrition aged 0-59 months, namely 2015 (5.5%),
2016 (4.6%) and 2017 (4.7%). Seen from the PSG
data, the trend of overnutrition is still fluctuating, so
there are still two possibilities for the next PSG result,
to go down/up.
Samarinda is one of the cities in Indonesia that
also contributes to the incidence of overweight
(BB/TB) in children under five, with a prevalence of
Hartati, D., Noviasty, R. and Susanti, R.
The Effect of Comprehensive Feeding Practices and Physical Activities on the Over-nutritional Status of Preschoolers in the Working Area of Juanda Community Health Center Samarinda.
DOI: 10.5220/0010758500003235
In Proceedings of the 3rd International Conference on Social Determinants of Health (ICSDH 2021), pages 53-63
ISBN: 978-989-758-542-5
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
53

3.0% in 2017, and ranks the 2nd highest obesity case
in children aged 0-4 years after Kukar, with 19 old
and new cases, the 4th highest obesity case at the age
of 5-9 years with a total of 11 cases, and the 3rd
highest according to the overall age group, with a
total of 2,242 cases (DKP Kaltim, 2018). The highest
incidence of overweight and obesity in children under
five in Samarinda in 2019 was in the Juanda
Community Health Center work area, with a total of
71 cases (DKK Samarinda, 2019).
In the current millennial era, coupled with the
enactment of the fourth industrial revolution (4.0)
which applies an all-machine system and the concept
of automation, it seems that it is increasingly
supporting humans to carry out less physical activity.
Related to this, WHO states that children aged 3-4
years should do more physical activity than sedentary
activities (eg sitting still or staring at a screen for a
long time). Guidelines for physical activity for
children this age are at least 180 minutes / day with
various types of physical activity and intensity
(WHO, 2019).
Previous studies with the aim of analyzing the
relationship between sleep duration, food intake and
physical activity with the incidence of obesity in
toddlers aged 3-5 years, the results showed that there
was a significant relationship between sleep duration,
food intake and physical activity with the incidence
of obesity in toddlers aged 3-5 years. years (p <
0.005) (Tristiyanti, Tamtomo and Dewi, 2018).
Several related studies also state that children's
eating behavior is strongly influenced by the family
environment, especially at the age of 3-5 years.
Where at this age the growth line in KMS begins to
look flat, but his/her cognitive and psychosocial
development is increasing rapidly (there is an
increase in comprehension and memory). So that
good habits that are applied since the child is at this
age will play an important role in the independence of
the child at a later age, including the application of a
good diet. This is also in line with the CDC (2020) on
Child Development (Mountin, 2020).
Changes in diet and physical activity are often the
result of environmental and social changes associated
with development and the lack of supportive policies
(WHO, 2020). Parents, especially mothers, play a
very important role in determining the diet of their
toddlers. Knowledge of maternal nutrition is very
influential in the selection of family food, which in
turn will affect the nutritional status of all family
members (especially toddlers) (Aditianti, Prihatini
and Hermina, 2016). The comprehensive feeding
practice carried out by the mother in question is
providing food with nutrition that is in accordance
with the child's needs, both in physical, mental and
emotional development, starting from preschool age
(Rysha, Gjergji and Ploeger, 2017).
In a preliminary survey conducted in Kemuning
Village, Arjasa District regarding the comprehensive
feeding practices of 5 mothers, the results showed that
on average the mother gave more restrictions to the
child if the child was sick, but when their returned to
health, the mother would again free the child's food
(Rahmawati, 2018). Based on the description above,
the researcher wants to conduct a study related to the
nutritional status of preschool aged children (3-5
years) in the working area of the Juanda Community
Health Center Samarinda with the independent
variables studied are the practice of feeding
comprehensive and physical activity of children.
Which the purpose of this study was to determine the
effect of the practice of comprehensive feeding and
physical activity on the nutritional status of preschool
age children (3-5 years) in the Working Area of
Juanda Community Health Center Samarinda.
2 RESEARCH METHOD
This type of this study was a analytic observational
with a matched case control design, namely a study
conducted retrospectively (looked at backwards
events) by identifying the case group and the control
group first, then examining the risk factors (in this
case the negative comprehensive feeding practices
and less physical activity). The independent variables
in this study was the comprehensive feeding practices
and physical activity, while the dependent variable
was the nutritional status of preschoolers.
The total population in this study were all pairs of
mothers and their preschool age children (3-5 years)
with an age calculation range seen from the month
and year of birth, with the upper limit being > 10
months in 2015 and the lower limit < 10 months in
2017 and with Zscore BMI/U - 2 SD, which was
recorded in the results of anthropometric
measurements of the posyandu in the Juanda Health
Center work area in 2019 with a total of 283 children.
Meanwhile, the population of cases with Zscore
BMI/U > + 2 SD is 25 children.
The time used in the implementation of this study
is mid-January - mid-March 2021. This research was
carried out in the Juanda Community Health Center
Work Area, Samarinda City, which consists of 2
Urban Village namely Air Hitam Urban Village and
Gunung Kelua Urban Village. Sampling was carried
out by non-probabilty sampling using a type of
purposive sampling technique (this sampling was
ICSDH 2021 - International Conference on Social Determinants of Health
54

based on subjective considerations from the
researchers themselves in accordance with the
inclusion and exclusion criteria that had been
determined and considered). For samples using the
formula Lemeshow as follows:
𝑛
𝑍
∝/
2𝑃
1𝑃
𝑍
𝑃
1 𝑃
𝑃
1 𝑃
𝑃
𝑃
Information:
n = Number of samples needed each
group (cases and controls)
Z_(1-∝/2) = Standard normal distribution value
at a certain 1.96 = 95% CI
significance degree with of 5%
Z_(1-β ) = The value of the standard normal
distribution at a certain (1.28 = test
power (power) by 90%)
P
1
= Estimated proportion of exposure in
the case group (ill) which is 0.191
(Setiawan, Machmud and Masrul,
2018)
P
2
= Estimated proportion of exposure in
the control group (not sick) which is
0.809 (Setiawan, Machmud and
Masrul, 2018)
P =
P =
,,
0,5
So, total of sample (n) in this study was:
1,96
2
0,5
10,5
1,28
0,191
1 0,191
0,809 1 0,809
0,191 0,809
11,52
To facilitate the calculation and processing of data
on the sample, the researchers rounded the total
sample into 12 toddlers (with BMI/U > 2 SD) as the
case group, and 24 toddlers (with BMI/U -2 SD to 2
SD) as the control group, with a comparison of the
samples used is 1: 2 (case group and control group)
and the total number of children under five is 36
children under five. The inclusion criteria are as
follows: Registered to be part of the Juanda
Community Health Center working area, Samarinda
City; Children aged 3-5 years whose BMI/U value is
seen from the Z score > + 2 SD (for the case group),
and Z score - 2 SD to + 2 SD according to BMI/U (for
the control group); Mother's occupation as a
Housewife (IRT) or taking care of her own children
at home; Mother is willing to be a respondent in this
study; Mentally and physically healthy both mother
and child under five. Then the exclusion criteria are
if: During the research, there is a family member (at
home) who is sick so that the mother's time is taken
up to take care of it; Die; or Resign.
Data collection using primary data and secondary
data. Primary data collected using the Comprehensive
Feeding Practices Questionnaire (CFPQ) and
Preschool-age Physical Activity Questionnaires (Pre-
PAQ), as well as secondary data through the latest
posyandu weighing records. Data analyzed by Chi
Square test and Odds Ratio with a significance value
of 0.05.
All questionnaires were distributed via WhatsApp
personal messages and filled out by mothers of
toddlers who were the research sample or may be
assisted by other family members, if at the time of
filling out the questionnaire the mother was not fluent
in using smartphones or lacked understanding in
answering the available questionnaires. This CFPQ
scoring system uses a Likert scale with a different
format, namely for item numbers 1-12 Never = 1,
Rarely = 2, Sometimes = 3, Often = 4, Always = 5.
While for item numbers 13-38 No Agree = 1,
Disagree = 2, Neutral = 3, Slightly Agree = 4, Agree
= 5. Then, there is a statement that ends with the R
logo, which indicates the statement is negative, so the
assessment uses an inverted Likert scale. The
measurement results from this CFPQ will be in the
form of categories, which are as follows (Warkentin
et al., 2016):
a. Negative feeding practices (if score < median)
b. Positive feeding practice (if score median)
The results of the questionnaire Pre-PAQ are
categorized into less physical activity (when the child
is active <180 minutes/day) and sufficient physical
activity (when the child is active 180 minutes/day)
(WHO, 2019) .
Validity test is the principle of instrument
reliability (questionnaire) which is measured and
observed for data collection. In making a decision on
the validity test, we must compare the r count with the
r table. If r count > r table then the question item from
the questionnaire is said to be valid, but if r count < r
table then the question item from the questionnaire is
said to be invalid. Reliability test is a test used to see
the stability of the instrument (questionnaire) in
collecting measurement results and research
observations. That is, in every measurement and
observation result with the same questionnaire
questions but at different times will get the same
results. (Donsu, 2017). The reliability test in this
study was carried out using the Alpha Cronbach
method. A variable in the questionnaire can be said to
be reliable if it produces Cronbach's Alpha (α) > 0.6
(Ghozali, 2011).
The Effect of Comprehensive Feeding Practices and Physical Activities on the Over-nutritional Status of Preschoolers in the Working Area
of Juanda Community Health Center Samarinda
55

3 RESULT AND DISCUSSION
3.1 Respondent Characteristics
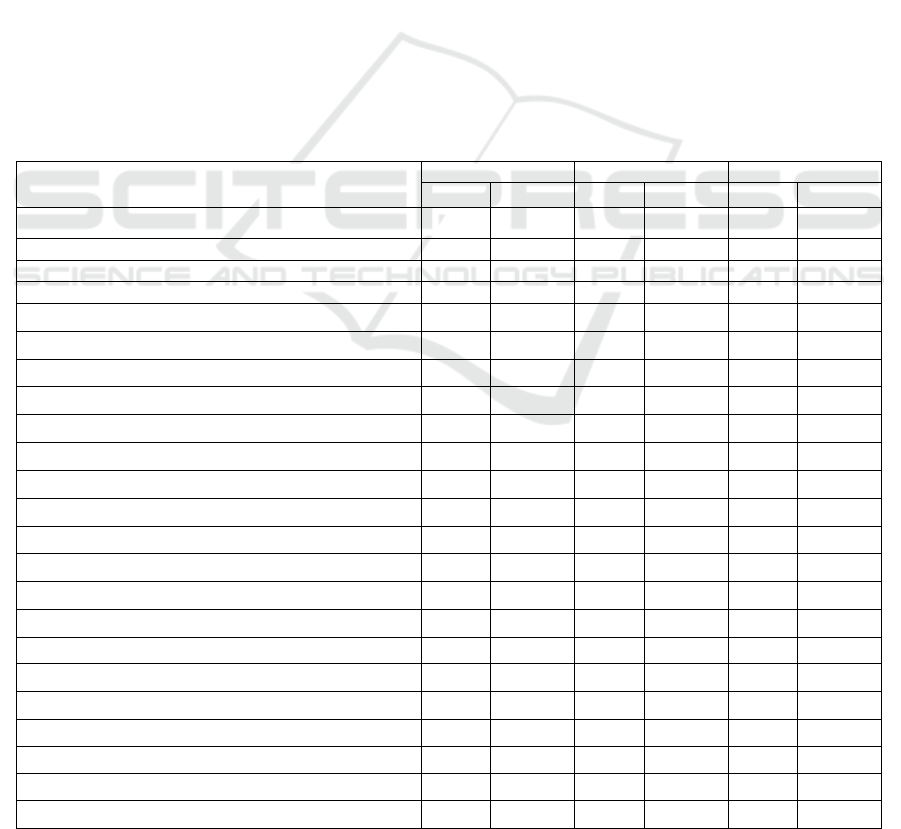
Table 1: Frequency Distribution of Respondents'
Characteristics on the Preschool Age Children in the
Working Area of the Juanda Community Health Center,
Samarinda.
Respondent
Characteristics
Child’s Nutritional Status
Over-Nutrition
n=12(%)
Normal
n=24(%)
Mother's Last Education
No school/Not
finished
elementary
school
1 (8,3%)
0 (0%)
Finished
Elementary
School
1 (8,3%)
1 (4,2%)
Finished Junior
High School
0 (0%) 5 (20,8%)
Finished Senior
Hi
g
h School
6 (50,0%) 10 (41,7%)
Graduated
(D3/S1/S2/S3)
4 (33,3%) 8 (33,3%)
Mother's Employment Status
Housewife 12 (100,0%) 24 (100,0%)
Etc 0 (0%) 0 (0%)
Number of Family Members in One House
3
p
eo
p
le 4
(
33,3%
)
2
(
8,3%
)
4 people 2 (16,7%) 12 (50,0%)
5 people 3 (25,0%) 6 (25,0%)
6 people 3 (25,0%) 4 (16,7%)
Child Gender
Male 5 (41,7%) 10 (41,7%)
Female 7
(
58,3%
)
14
(
58,3%
)
Source: Primary Data, 2021
Based on the table 1 above, information can be
obtained that most of the mothers last education in the
sample group was high school graduates, namely in
the group of preschool age children who experienced
well-nutrition/normal (41.7%) and over-nutrition
(50.0%) in the Juanda Health Center Samarinda. The
occupational status of mothers from both groups
(both normal and over-nutrition) are housewives
(100%).
The majority of family members in one house in
the group of preschool-aged children with normal
status are 4 family members (50.0%) and in the group
of preschool-aged children with over-nutrition status
are 3 family members (33.3%). Then, the majority of
respondents had preschool-aged children who were
female in both groups, namely the normal group
(58.3%) and the over-nutrition group (58.3%).
This research was conducted in the working area
of Juanda Community Health Center Samarinda,
which is located in the Samarinda Ulu District. The
working area of the Juanda Samarinda Health Center
consists of 2 Urban Village, namely Air Hitam Urban
Village and Gunung Kelua Urban Village. Air Hitam
and Gunung Kelua Urban Villages are geographically
next to each other (to the east, Air Hitam Urban
Village is Gunung Kelua Urban Village, and to the
west Gunung Kelua Urban Village is Air Hitam
Urban Village). Gunung Kelua Urban Village is
located in the heart of the capital city of East
Kalimantan Province where the centers of community
activities such as economics (shopping centers) and
academics (colleges and schools) are located in this
area.
In line with the general description of the location
of this study, in general the problems of overweight
and obesity are supported by an increase in intake of
energy-dense foods (high in fat and sugar) and an
increase in sedentary activity due to the increasing
number of sedentary jobs, changes in transportation
modes, and increasing urbanization. (WHO, 2020).
Likewise, the description of the location of this study
which is overall in an urban area which is an
obesogenic environment (an environment with a
sedentary lifestyle and lots of fast food available with
a relatively close distance from the house making it
easier to access).
In line with the results of this study, the research
of Schrempft et al. (2015) showed that preschoolers
with obesogenic living environments, consumed less
vegetables and fruits, compared to consuming high-
energy snacks and drinking sugary drinks. In
addition, the behavior of children in choosing their
food is also inseparable from what they like and have
known before. Therefore, the experience of children
from an early age will greatly affect their food choices
and preferences later (Scaglioni et al., 2011).
The quality of food intake at preschool age is very
dependent on parents (especially mothers). All
supplies, serving, and eating habits at home will
affect children's consumption patterns. There are
several factors that influence parental feeding to their
children, including economic, socio-cultural,
educational, environmental, and maternal age
(Sulistyoningsih, 2011). The results of research
Farhan (2014) state that, one of the factors that
determine whether or not someone easily absorbs and
understands the nutritional knowledge they get is the
level of education.
The characteristics of the research results in table
1 show the description of the last education of the
majority of mothers who graduated from senior high
ICSDH 2021 - International Conference on Social Determinants of Health
56
school, namely as many as 16 people (44.5%). At
least, the majority of mothers have completed their
education to fulfill the 12-year compulsory education
program. From these results, it can also be seen that
it is precisely at the level of high school graduation
that on average they have children with more
nutritional problems. This shows that in fact not all
highly educated people will have good knowledge as
well, or knowledge and higher education are not
always directly proportional to that person's attitude
or behavior.
The results of the study in the table 1 state that the
majority of the number of family members in one
house in the group of preschool age children with
good nutritional status are 4 family members (50.0%)
and in the group of preschool age children with more
nutritional status are 3 family members (33.3%).
Djala research (2016) says that the amount of food
and the frequency of food consumed by each family
member is influenced by the size of the number of
family members.
The results of the study itn table 1 state that the
majority of children with overnutrition status are
female, as many as 7 children (58.3%). There are
several factors that can be the cause of more girls than
boys with more nutritional status, one of which is that
women's metabolism is slower than men's. Men have
a 10% higher basal metabolic rate than women,
because women tend to convert food into fat, whereas
in men more food is converted into muscle and as a
ready-to-use energy reserve. (Lestari, 2017).
In addition to differences in basal metabolic rate,
it was also stated in Lestari's research (2017) that
lighter physical activity in women will certainly be a
triggering factor for fat accumulation in the body as
well. In line with the previous research, the results of
the analysis in this study also showed that more or
less physical activity occurred in children of the
female sex than boys.
3.2 Univariat
3.2.1 Frequency Distribution of
Respondents based on Comprehensive
Feeding Practice
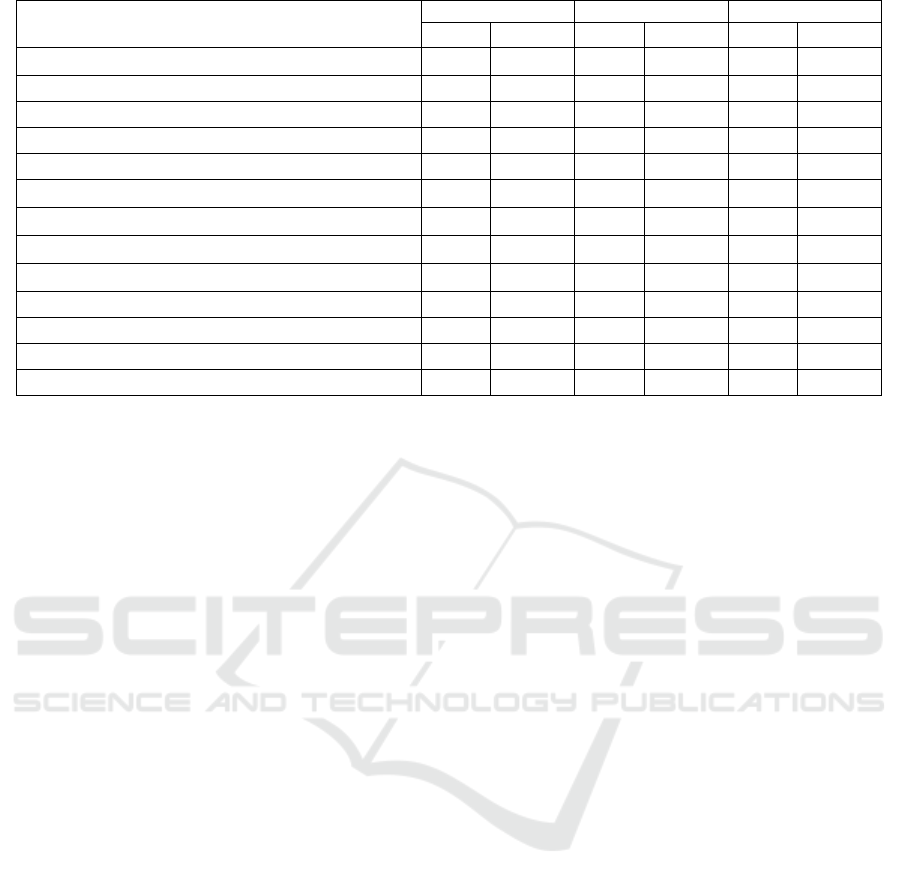
Table 2: Frequency Distribution of Respondents Based on Comprehensive Feeding Practices.
Category
Comprehensive Feeding Practices
Ove
r
-Nutrition Normal Total
n=12 % n=24 % n=36 %
Monitoring
Negative Feeding Practices 9 75,0% 6 25,0% 15 41,7%
Positive Feeding Practices 3 25,0% 18 75,0% 21 58,3%
Total 12 100,0% 24 100,0% 36 100,0%
Emotion Regulation
Negative Feeding Practices
10 83,3% 4 16,7% 14 38,9%
Positive Feeding Practices
2 16,7% 20 83,3% 22 61,1%
Total
12 100,0% 24 100,0% 36 100,0%
Food as a Reward
Negative Feeding Practices
8 66,7% 8 33,3% 16 44,4%
Positive Feeding Practices
4 33,3% 16 66,7% 20 55,6%
Total
12 100,0% 24 100,0% 36 100,0%
Child Control
Negative Feeding Practices
10 83,3% 4 16,7% 14 38,9%
Positive Feeding Practices
2 16,7% 20 83,3% 22 61,1%
Total
12 100,0% 24 100,0% 36 100,0%
Healthy Eating Guide
Negative Feeding Practices
9 75,0% 5 20,8% 14 38,9%
Positive Feeding Practices
3 25,0% 19 79,2% 22 61,1%
Total
12 100,0% 24 100,0% 36 100,0%
Pressure to Eat
Negative Feeding Practices
8 66,7% 9 37,5% 17 47,2%
Positive Feeding Practices
4 33,3% 15 62,5% 19 52,8%
The Effect of Comprehensive Feeding Practices and Physical Activities on the Over-nutritional Status of Preschoolers in the Working Area
of Juanda Community Health Center Samarinda
57
Category
Comprehensive Feeding Practices
Ove
r
-Nutrition Normal Total
n=12 % n=24 % n=36 %
Total
12 100,0% 24 100,0% 36 100,0%
Restriction for Weight
Negative Feeding Practices
6 50,0% 5 20,8% 11 30,6%
Positive Feeding Practices
6 50,0% 19 79,2% 25 69,4%
Total
12 100,0% 24 100,0% 36 100,0%
Healthy Environment
Negative Feeding Practices
9 75,0% 3 12,5% 12 33,3%
Positive Feeding Practices
3 25,0% 21 87,5% 24 66,7%
Total
12 100,0% 24 100,0% 36 100,0%
Arrangements
Negative Feeding Practices
10 83,3% 5 20,8% 15 41,7%
Positive Feeding Practices
2 16,7% 19 79,2% 21 58,3%
Total
12 100,0% 24 100,0% 36 100,0%
Source: Primary Data, 2021
Based on the table 2, information can be obtained that
in the monitoring category in the characteristics of
parental feeding practices to their preschool age
children, there are 9 respondents (75.0%) in the case
group and 6 respondents (25.0%) in the control group
who carry out monitoring characteristics negatively.
In the emotion regulation category, there were 10
respondents (83.3%) in the case group and 4
respondents (16.7%) in the control group who carried
out negative emotion regulation characteristics. In the
food as a reward category, there were 8 respondents
(66.7%) in the case group and 8 respondents (33.3%)
in the control group who carried out the
characteristics of the food as a reward negatively. In
the child control category, there were 10 respondents
(83.3%) in the case group and 4 respondents (16.7%)
in the control group who had negative child control
characteristics.
In the healthy eating guide category, there were 9
respondents (75.0%) in the case group and 5
respondents (20.8%) in the control group who carried
out the characteristics of the healthy eating guide
negatively. In the restriction for weight category,
there were 8 respondents (66.7%) in the case group
and 9 respondents (37.5%) in the control group who
carried out the characteristics of restriction for weight
negatively. In the weight control category, there were
6 respondents (50.0%) in the case group and 5
respondents (20.8%) in the control group who had
negative weight control characteristics. In the healthy
environment category, there were 9 respondents
(75.0%) in the case group and 3 respondents (12.5%)
in the control group who carried out healthy
environment characteristics negatively. In the
arrangements category, there were 10 respondents
(83.3%) in the case group and 5 respondents (20.8%)
in the control group who had negative arrangements
characteristics.
Positive feeding practices are feeding practices
carried out by parents to their children by paying
attention to the interaction between parents and
children during the feeding process and in accordance
with balanced nutrition or nutritional needs for the
child's body, while negative feeding practices are the
opposite. Overall, as seen from table 2, the most
negative comprehensive feeding practices carried out
by mothers in preschool aged children (3-5 years) in
the Working Area of Juanda Community Health
Center Samarinda is the "Pressure to Eat" category
with a total of 17 respondents (47.2% ) and the least
negative is the “Restriction for Weight” category with
a total of 11 respondents (30.6%). The results of the
study in table 2 for the "monitoring" category show
that mothers of preschool-aged children who are
overweight are still relatively lacking in monitoring
food intake consumption in children (with a
percentage of 75%), so that the nutritional status
needed by children is not met properly. Preschool age
children are able to choose and know what food they
want to eat and what they like, so this period can also
be referred to as the transition period for children
from passive consumers to active consumers.
However, they do not understand to choose which
foods are good and which are not good for health, so
parents in this case play an important role in being
able to control their children's eating choices in order
to win nutritionally balanced food choices.
(Permenkes RI No 41, 2014).
The results of the "emotional" category research
show that mothers of preschool-aged children who
ICSDH 2021 - International Conference on Social Determinants of Health
58

experience over-nutrition relatively often use food as
an ingredient to divert children's feelings when
children are angry or upset, in other words, parents
use food or drink as a regulator of children's emotions
(by percentage of 83.3%). When a child feels angry
or upset, making his heart calm first and then helping
him to talk about his feelings to the mother so that the
child can find ways to deal with his emotions will be
much better, than having to involve food
(Misnadiarly, 2007).
The results of the "food as a reward" category
research show that mothers of preschool-aged
children who are over-nutrition still relatively often
use their children's favorite food or drink as a reward
for good behavior that has been carried out by
children, usually in this case preschoolers prefer
foods and drinks high in sugar (ie with a percentage
of 66.7%). In appreciating a child's good behavior and
stopping his bad behavior, giving snacks as a gift for
him is not the right solution to appreciate his
behavior. Looking for other ways, such as praising or
thanking children for their good behavior will be
better (Misnadiarly, 2007).
The results of the "child control" category
research show that mothers of preschool-aged
children who experience over-nutrition are still
relatively lacking in controlling/controlling children's
eating behavior and interacting in their feeding to
maintain children's consumption patterns so that they
are not arbitrary in choosing and consuming their
food (with the percentage of 83.3%). An unhealthy
child's diet can indeed lead to weight gain, but
explicitly forbidding him to eat such foods is also not
good. If children are too restricted/forbidded, they can
eat more quietly behind their parents' back. So the
best way is to control access to food like this at home.
For example, when mothers shop for their daily food
needs, mothers can pay more attention to preferences
for food and snacks to be purchased (Misnadiarly,
2007).
The results of the research category "guidance for
healthy eating" show that mothers of preschool-aged
children who experience over-nutrition are still
relatively lacking in carrying out healthy eating
guidelines (such as telling, clearly describing,
discussing, offering, and/or exemplifying good eating
patterns) to their children (ie with a percentage of
75%). When parents want their children to live
healthy, then parents must be the main example in
their lives. Parents who have a good diet will also
form a good diet in their children which can continue
until they grow up (Misnadiarly, 2007). In line with
this theory, the research conducted by
Prasetyaningrum et al. (2016) also mentions that
parental behavior plays a role in shaping eating
behavior in children. It is known that preschool
children (3-5 years) who live with mothers with
unhealthy eating behavior are 2.45 times more likely
to be obese.
The results of the "pressure to eat" category of
research show that mothers of preschool-aged
children who experience over-nutrition are still
relatively feeding their children in a pressing or
coercive style, so that children eat more food,
especially when it is time to eat, usually done to
increase the child's weight (ie with a percentage of
66.7%). As parents (especially mothers who take care
of children intensely) must be able to realize
nutritional needs for children in accordance with the
activities they do everyday. If the child is full enough,
the mother should not get used to forcing the child to
continue eating or to always finish the contents of his
plate (Misnadiarly, 2007).
The results of the research in the "restriction for
weight" category show that mothers of preschool-
aged children who are over-nutrition are still
relatively unable to control/regulate their children's
food intake to reduce or maintain their child's weight
(that is, with a percentage of 50%). Getting used to
eating regularly at predetermined hours can prevent
children from obesity. But it must also be
remembered that giving snacks that are high in sugar,
fat and calories too often can also lead to obesity.
Thus, making a commitment within the family to
carry out healthy habits and determine the pattern and
adhere to it, will make children interested in doing it
and they will not feel alienated because of the same
treatment for all family members including mothers
(Misnadiarly, 2007).
The results of the "healthy environment" category
research show that mothers of preschool-aged
children who experience over-nutrition are still
relatively lacking in providing healthy food and not a
few of them actually provide more stock of unhealthy
snacks at home, even though the family is the most
important factor in determining children's diet (ie
with a percentage of 75%). Children usually do not
shop for their own food needs, parents are fully
responsible for the stock of healthy food available at
home. For mothers, it is recommended that when
shopping, you should choose fruits and vegetables as
a snack supply at home and avoid choosing fast food,
limit the purchase of sugary drinks because they only
provide less nutrition than the high calories they have,
and choose recipes and cooking methods with the use
of as little fat as possible (such as baking/boiling)
(Misnadiarly, 2007).
The Effect of Comprehensive Feeding Practices and Physical Activities on the Over-nutritional Status of Preschoolers in the Working Area
of Juanda Community Health Center Samarinda
59
The results of the research in the “arrangements”
category show that mothers of preschool-aged
children who are more over-nutrition are still
relatively insensitive to the importance of their role as
mothers in regulating their children's consumption
patterns (ie with a percentage of 83.3). Of the 9
variables of comprehensive feeding practices studied,
the variable that was mostly carried out on preschool-
aged children (3-5 years) in the Working Area of
Juanda Community Health Center Samarinda with a
negative category (in case and control groups) was the
"coercive" variable, namely 17 respondents (47.2%).
Meanwhile, the variable that was the least negative (in
both case and control groups) was the “weight
control” variable, namely 11 respondents (30.6%).
3.2.2 Frequency Distribution of
Respondents based on Children's
Physical Activity
Table 3: Frequency Distribution of Respondents Based on
Children's Physical Activity.
Category
Children’s
Physical
Activity
Over-
Nutrition
Normal Total
n=
12
%
n=
24
%
n=
36
%
Less 9 75% 2 8,3% 11 30,6%
Sufficient 3 25% 22 91,7% 25 69,4%
Total 12 100% 24 100% 36 100%
Source: Primary Data, 2021
In table 3 above, information can be obtained that
from 12 preschool-aged children with over-
nutritional status as many as 9 children (75%) do
physical activity in the less category and 3 children
(25%) do physical activity in the sufficient category.
Meanwhile out of 24 children with normal nutritional
status, 2 children (8.3%) did physical activity in the
less category and 22 children (91.7%) did physical
activity in the sufficient category.
From table 3, information can also be obtained
that the physical activity of preschoolers (3-5 years)
in the Working Area of the Juanda Samarinda Health
Center is on average in the sufficient category, as
many as 25 children (69.4%) have sufficient physical
activity category. It's just that in children with more
nutritional status, the majority of preschoolers still
have a category of less physical activity, as many as
9 children (75%). In line with the results of this study,
the research of Carson et al. (2017) also found that
children with over-nutritional status had less physical
activity than children with normal nutritional status.
The results of this study also showed that children
with normal nutritional status but classified as having
less physical activity were 2 children (8.3%) out of 36
children (100%). This shows that physical activity is
not also the only factor that influences the incidence
of overnutrition. Research conducted by Wilks et al.
(2011) actually get the results that there is no
significant relationship between physical activity and
body fat mass. In the study, physical activity was not
the main determinant of unhealthy weight gain in
children.
3.3 Bivariat
3.3.1 The Effect of Comprehensive Feeding
Practices on over Nutritional Status of
Preschool Age Children in the
Working Area of Juanda Community
Health Center Samarinda
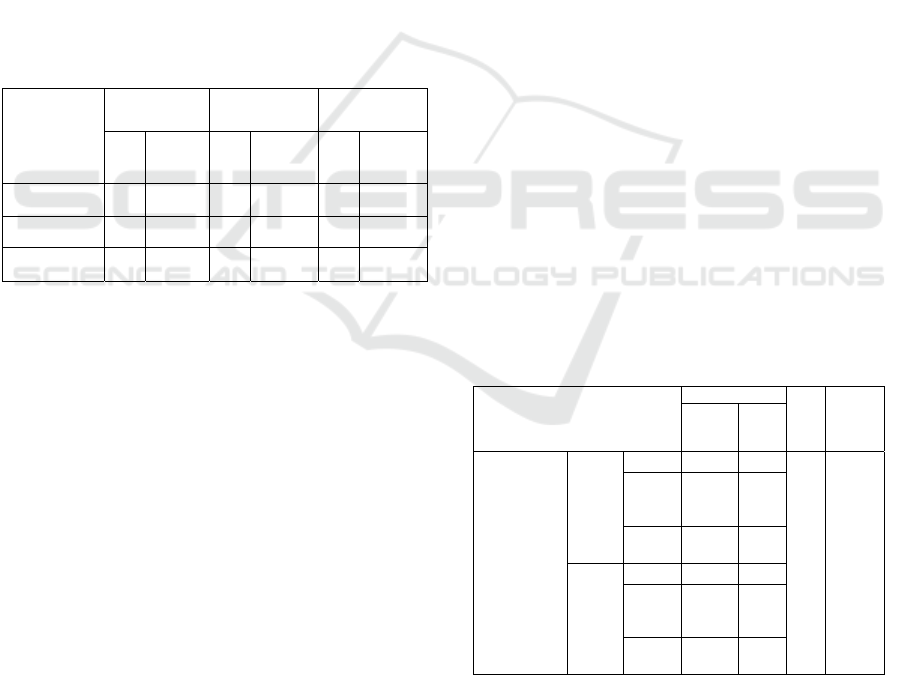
Based on table 4, it can be seen that of the 12
respondents who have preschool-aged children with
over-nutritional status, there are 11 respondents
(91.7%) of whom practice comprehensive feeding in
the negative category and 1 respondent (8.3%) does
comprehensive feeding practices with positive
category. Meanwhile, of the 24 respondents who had
preschool-aged children with good nutritional status,
7 respondents (29.2%) does comprehensive feeding
practices with negative category and 17 respondents
(70.8%) does comprehensive feeding practices with
positive category.
Table 4: The Effect of Comprehensive Feeding Practices on
Over Nutritional Status of Preschool Age Children in the
working area of Juanda Community Health Center
Samarinda.
Nutritional Status
P
Value
OR
(CI:95%)
Bottom-
U
p
Over-
Nutrition
Normal
Comprehensive
Feeding
Practices
Negative
Feeding
Practices
Count 11 7
0,001
26,714
(2,877 –
248,023)
% within
Status
Gizi
91.7% 29.2%
Expected
Count
6.0 12.0
Positive
Feeding
Practices
Count 1 17
% within
Status
Gizi
8.3% 70.8%
Expected
Count
6.0 12.0
Source: Primary Data, 2021
Based on the results of the statistical test, the P
value (P Value) was 0.001. Because the P Value
(significance) is less than 0.05, it can be concluded
that there is an effect of comprehensive feeding
practices on the nutritional status of preschool age (3-
ICSDH 2021 - International Conference on Social Determinants of Health
60
5 years) in the Working Area of Juanda Community
Health Center Samarinda, with an Odds Ratio (OR)
of 26.714 OR > 1) which means that there is a
possibility that a child with a negative comprehensive
feeding practice will have a 26.7 times greater risk of
experiencing overnutrition than a child with a positive
comprehensive feeding practice..
In line with the results of this study, other studies
also state that the practice of caring for toddlers and
mother's knowledge affect the nutritional status of
toddlers (Masita, Biswan and Puspita, 2018). The
results of other studies that support also state that
there is a significant relationship between eating
patterns and the nutritional status of children under
five (P Value = 0.014) (Pratiwi, Masrul and Yerizel,
2016). How parents apply their parenting style to their
children, will also determine what their child's life
will be like in the future, and this is in line with the
research of Suratman et al. (2018). Thus, parents
(especially in this case mothers) play an important
role in the growth and development of children
through parenting practices and the provision of
nutrients to children.
Without having to look at whether children are at
risk of being overweight or even having an ideal
weight, paying attention to the food you eat so that
you can consistently maintain an ideal weight is a
good example for children. So, from here, mothers
can invite their children to participate in doing
healthy habits together. (Misnadiarly, 2007).
3.3.2 The Effect of Physical Activity on over
Nutritional Status of Preschool Age
Children in the Working Area of
Juanda Community Health Center
Samarinda
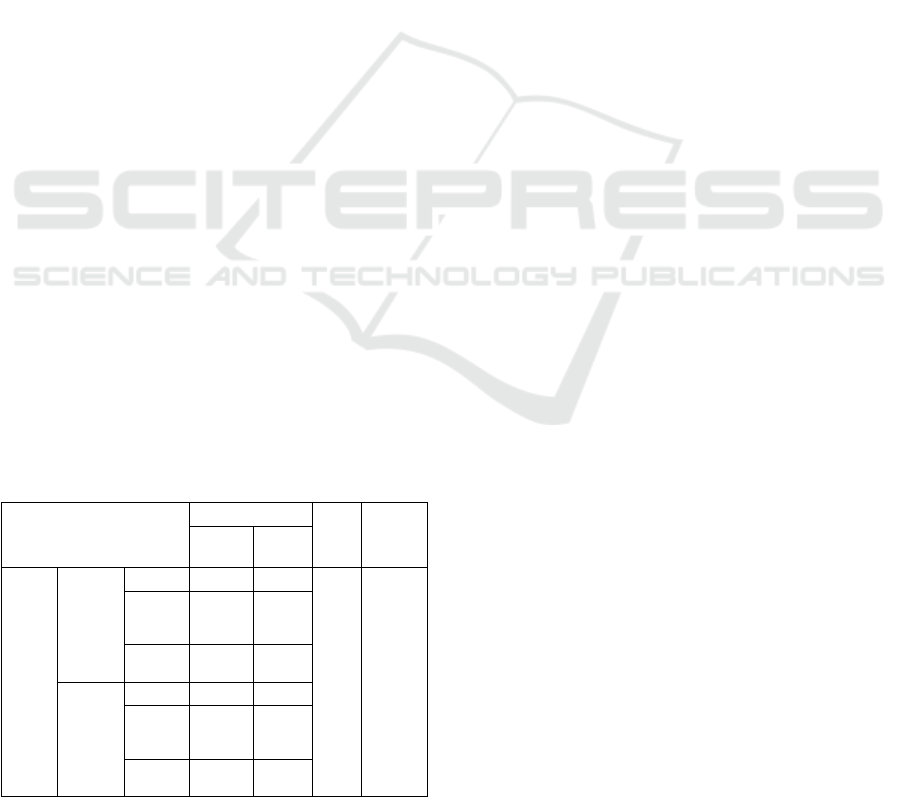
Table 5: The Effect of Physical Activity on Over
Nutritional Status of Preschool Age Children in the working
area of Juanda Community Health Center Samarinda.
Nutritional Status
P
Value
OR
(CI:95%)
Bottom-
U
p
Over-
Nutrition
Normal
Physical
Activity
Less
Count 9 2
0,000
33,000
(4,695 –
231,956)
% within
Status
Gizi
75.0% 8.3%
Expected
Count
3.7 7.3
Sufficient
Count 3 22
% within
Status
Gizi
25.0% 91.7%
Expected
Count
8.3 16.7
Source: Primary Data, 2021
Based on the results of the statistical test on the
table 5, the P value was 0.000 (<0.05). Thus, it can be
concluded that there is an effect of physical activity
on the over-nutritional status of preschool aged
children (3-5 years) in the Working Area of Juanda
Community Health Center Samarinda, with an Odds
Ratio (OR) of 33 (OR > 1) which means that there is
a possibility that a child experiencing over-nutrition
due to lack of physical activity which is 33 times
greater than if the child has sufficient physical
activity. In line with the results of this study, the
research of Rahmah et al. (2019) also stated that
physical activity (p= 0.004) and physical activity
parenting (p= 0.01) were the most influential risk
factors for the incidence of over-nutrition in
preschool children.
The results show that almost all children spend
their time eating in front of a screen (be it a
smartphone or television). Habits like this can make
children consume food unconsciously how much
food they have eaten and make children eat in a hurry
(Misnadiarly, 2007). In addition, parents also very
rarely bring their children to play in open spaces/areas
such as riverbanks, nature reserves, environmental
parks/tourist parks, or even playgrounds to increase
children's activities.
Children, especially preschoolers, should not
spend their time solely on sedentary activities, such
as watching television coupled with excessive
snacking, playing video games and the like, or just
lying in bed for more than 60 minutes. Spending time
with active activities is very important for
preschoolers, there are at least 180 minutes per day to
do physical activity of any intensity which 60 minutes
in it includes doing moderate to strenuous physical
activity (energetic games) such as running, cycling
and dancing, that makes children sweating and
panting (WHO, 2019).
The results of this study also show that on average
children need someone to accompany them to be
motivated to play. Meanwhile, on the other hand, the
results of this study also show that the time used by
children to play outdoors (whether on weekends or
weekdays) is very little or even no time for children
to play outdoors, especially for children with over-
nutritional status, even in good weather conditions.
So that children's activities at home are sufficient
limited and more use of screens or smartphones.
Parents are also responsible for the habits of
activities carried out by children. Parents must have a
"supportive" attitude for every activity children. In
supporting the activities carried out by children,
parents can make family policies/commitments to be
obeyed and carried out by every family member,
The Effect of Comprehensive Feeding Practices and Physical Activities on the Over-nutritional Status of Preschoolers in the Working Area
of Juanda Community Health Center Samarinda
61

including parents. Some examples of good policies to
do are parents being a real example for every activity
both indoors/outdoors, encouraging children to try
new activities and responding positively when they
do it, and providing fun and interesting activities
every day (Nemours Health & Prevention Services,
2013).
When children are active and there are dangers of
safety problems and/or other problems (such as mud,
fights over fighting over toys with friends, etc.),
parents need to direct their children well and slowly
so that children return to playing in safe activities or
invite them to discussion about what to do when faced
with it. Parents also need to avoid using physical
activity as a punishment. (Nemours Health &
Prevention Services, 2013).
4 CONCLUSIONS
After conducting research on 36 respondents to
housewives (IRT) who have preschool aged children
(3-5 years) in the working area of Juanda Health
Center Samarinda, it can be concluded that there is an
effect of the practice of comprehensive feeding on the
nutritional status of preschool children (3-5 years) in
the working area of the Juanda Health Center,
Samarinda, with a P Value of 0.001 (<0.05) and an
Odds Ratio of 26.714 (OR > 1) which that is, children
with mothers who practice negative comprehensive
feeding have a 26,714 times greater risk of
experiencing over-nutrition compared to children of
mothers who practice positive feeding. Parents need
to provide an "exemplary" attitude in terms of eating
behavior, for example if the mother wants her child to
eat healthy food, the mother also needs to set an
example and start as early as possible to create a
"good habit/activity".
There is an effect of physical activity on the
nutritional status of preschool children (3-5 years) in
the working area of Juanda Community Health Center
Samarinda, with a P Value of 0.000 (<0.05) and an
Odds Ratio of 33 (OR> 1) which means, Children
with less physical activity have a 33 times greater risk
of experiencing over-nutrition than children of
mothers who do quiet physical activity. It is
recommended for mothers to be more supportive of
children in moving more actively by bringing
children to open space areas regularly (at least 180
minutes a day for children to be active).
REFERENCES
Aditianti, A., Prihatini, S. and Hermina, H. (2016)
‘Pengetahuan, Sikap dan Perilaku Individu Tentang
Makanan Beraneka Ragam sebagai Salah Satu
Indikator Keluarga Sadar Gizi (KADARZI)’, Buletin
Penelitian Kesehatan, 44(2), pp. 117–126. doi:
10.22435/bpk.v44i2.5455.117-126.
Carson, V. et al. (2017) ‘Systematic review of the
relationships between physical activity and health
indicators in the early years (0-4 years)’, BMC Public
Health. Available at:
https://bmcpublichealth.biomedcentral.com/articles/10
.1186/s12889-017-4860-0.
Djala, P. N. V. (2016) Hubungan Antara Status Sosial
Ekonomi Terhadap Obesitas Sentral Pada Orang
Dewasa Sehat di Desa Kepuharjo, Kecamatan
Cangkringan, Yogyakarta. Universitas Sanata Dharma
Yogyakarta.
Donsu, J. D. T. (2017) Metodologi Penelitian Keperawatan.
Yogyakarta: Pustaka Baru.
Farhan, M. (2014) Hubungan Pengetahuan Ibu Rumah
Tangga Tentang Gizi Seimbang Dan Perilaku
Pemenuhan Gizi Pada Balita Usia 3-5 Tahun Di Desa
Banjarsari Kec Ciawi Kabupaten Bogor, Skripsi
Keperawatan. Universitas Islam Negeri Syarif
Hidayatullah Jakarta.
Ghozali, I. (2011) Aplikasi Analisis Multivariate Dengan
Program IBM SPSS 19. Semarang: Badan Penerbit
Universitas Diponegoro.
Kemenkes RI (2020) ‘Gizi Saat Remaja Tentukan Kualitas
Keturunan’, Biro Komunikasi dan Pelayanan
Masyarakat, Kemenkes RI. Available at:
https://www.kemkes.go.id/article/view/20012600004/
gizi-saat-remaja-tentukan-kualitas-keturunan.html.
Kemenkes RI, B. P. dan P. (Balitbang) (2019) ‘Laporan
Hasil Riset Kesehatan Dasar (Riskesdas) Indonesia
tahun 2018’, Riset Kesehatan Dasar 2018, pp. 182–183.
Lestari (2017) ‘Hubungan Pola Makan Dengan Kejadian
Obesitas Pada Anak Usia 3-8 Tahun Di TK Dan SD
Budi Mulia Dua Seturan Yogyakarta’, Naskah
Publikasi, p. 4.
Masita, M., Biswan, M. and Puspita, E. (2018) ‘Pola Asuh
Ibu dan Status Gizi Balita’, Quality : Jurnal Kesehatan,
12(2), pp. 23–32. doi: 10.36082/qjk.v12i2.44.
Misnadiarly (2007) Obesitas Sebagai Faktor Risiko
Beberapa Penyakit. 1st edn. Jakarta: Pustaka Obor
Populer.
Mountin, J. W. (2020) ‘Child Development’. Amerika
Serikat: Centers for Disease Control and Prevention.
Available at:
https://www.cdc.gov/ncbddd/childdevelopment/facts.h
tml.
Nemours Health & Prevention Services (2013) ‘Best
Practices for Physical Activity, v3’. Available at:
https://d3knp61p33sjvn.cloudfront.net/media-
resources/ECELC/C2P2/LS3/ECE_Program_Participa
nts/English_PhysicalActivityGuide_FINAL.pdf.
Permenkes RI No 41 (2014) ‘Pedoman Gizi Seimbang’.
Available at:
ICSDH 2021 - International Conference on Social Determinants of Health
62

http://kesmas.kemkes.go.id/perpu/konten/permenkes/p
mk-no.-41-ttg-pedoman-gizi-seimbang.
Prasetyaningrum, Y. I., Kertia, N. and Gunawan, I. M. A.
(2016) Home Food Environment Sebagai Faktor Risiko
Kegemukan Pada Anak Prasekolah Di Kota
Yogyakarta. Universitas Gadjah Mada. Available at:
http://etd.repository.ugm.ac.id/home/detail_pencarian/
95143.
Pratiwi, T. D., Masrul, M. and Yerizel, E. (2016)
‘Hubungan Pola Asuh Ibu dengan Status Gizi Balita di
Wilayah Kerja Puskesmas Belimbing Kota Padang’,
Jurnal Kesehatan Andalas, 5(3), pp. 661–665. doi:
10.25077/jka.v5i3.595.
Rahmah, N. D., Ardiaria, M. and Dieny, F. F. (2019) ‘Pola
Asuh Aktivitas Fisik Terhadap Risiko Kejadian Gizi
Lebih Pada Anak Prasekolah Di Kecamatan Ngesrep
Dan Tembalang, Semarang’, Gizi Indonesia, 42(1), p.
1. doi: 10.36457/gizindo.v42i1.363.
Rahmawati, L. W. (2018) Hubungan Praktik Komprehensif
Pemberian Makanan Dengan Status Gizi Anak
Preschool Di Desa Kemuning Kecamatan Arjasa
Kabupaten Jember. Jember. Available at:
https://repository.unej.ac.id/bitstream/handle/1234567
89/91072/Laili Wiji Rahmawati-
152310101027.pdf?sequence=1.
Rysha, A., Gjergji, T. M. and Ploeger, A. (2017)
‘Nutritional status of preschool children attending
kindergartens in Kosovo’, Journal of Health,
Population and Nutrition. Journal of Health, Population
and Nutrition, 36(1). doi: 10.1186/s41043-017-0105-1.
Scaglioni, S. et al. (2011) ‘Determinants of children’s
eating behavior’, American Journal of Clinical
Nutrition, 94(6), pp. 2006–2011. doi:
10.3945/ajcn.110.001685.
Schrempft, S. et al. (2015) ‘The obesogenic quality of the
home environment: Associations with diet, physical
activity, TV viewing, and BMI in preschool children’,
PLoS ONE, 10(8), pp. 1–17. doi:
10.1371/journal.pone.0134490.
Setiawan, E., Machmud, R. and Masrul (2018) ‘Artikel
Penelitian Faktor-Faktor yang Berhubungan dengan
Kejadian Stunting pada Anak Usia 24-59 Bulan di
Wilayah Kerja Puskesmas Andalas Kecamatan Padang
Timur Kota Padang Tahun 2018’, jurnal.fk.unand, 7(2),
pp. 275–284.
Sulistyoningsih, H. (2011) Gizi Untuk Kesehatan Ibu dan
Anak. Yogyakarta: Graha Ilmu.
Suratman, P. V. G., Triandhini, R. L. N. K. R. and
Nusawakan, A. W. (2018) ‘Parenting System Towards
Feeding the Children of Elementary Students at Binaus
Village Pola Asuh Orang Tua Terhadap Pemberian
Makan Pada Anak Usia Sekolah Dasar di Desa Binaus’,
pp. 22–28.
Tristiyanti, W. F., Tamtomo, D. G. and Dewi, Y. L. R.
(2018) ‘Analisis Durasi Tidur, Asupan Makanan, dan
Aktivitas Fisik sebagai Faktor Risiko Kejadian
Obesitas pada Balita Usia 3-5 Tahun’, Sari Pediatri,
20(3), p. 178. doi: 10.14238/sp20.3.2018.178-84.
UNICEF (2019) Children , food and nutrition. Edited by S.
Wauchope and et al. New York: United Nations
Children’s Fun (UNICEF). Available at:
https://www.unicef.org/media/61871/file/SOWC-
2019.pdf.
UNICEF, WHO and The World Bank (2019) Levels and
Trends in Child Malnutrition: Key Findings Of The
2019 Edition. Geneva. Available at:
https://www.who.int/nutgrowthdb/jme-2019-key-
findings.pdf?ua=1.
Warkentin, S. et al. (2016) ‘Validation of the
comprehensive feeding practices questionnaire in
parents of preschool children in Brazil’, BMC Public
Health. BMC Public Health, 16(1), pp. 1–12. doi:
10.1186/s12889-016-3282-8.
WHO (2019) WHO Guidelines on physical activity,
sedentary behaviour, World Health Organization.
Available at:
https://apps.who.int/iris/bitstream/handle/10665/32514
7/WHO-NMH-PND-2019.4-
eng.pdf?sequence=1&isAllowed=y%0Ahttp://www.w
ho.int/iris/handle/10665/311664%0Ahttps://apps.who.i
nt/iris/handle/10665/325147.
WHO (2020) ‘Obesity and Overweight’, World Health
Organization, 1 April. Available at:
https://www.who.int/news-room/fact-
sheets/detail/obesity-and-overweight.
Wilks, D. C. et al. (2011) ‘Objectively measured physical
activity and fat mass in children: A bias-adjusted meta-
analysis of prospective studies’, PLoS ONE, 6(2). doi:
10.1371/journal.pone.0017205.
The Effect of Comprehensive Feeding Practices and Physical Activities on the Over-nutritional Status of Preschoolers in the Working Area
of Juanda Community Health Center Samarinda
63
