
Detection of Coughing and Respiratory Sensing in Conversational
Speech
Venkata Srikanth Nallanthighal
1,2
, Aki Harm
1
, Ronald Rietman
1
and Helmer Strik
2
1
Philips Research, Eindhoven, The Netherlands
2
Centre for Language Studies (CLS), Radboud University Nijmegen, The Netherlands
Keywords: Speech Breathing, Signal Processing, Deep Neural Networks, Respiratory Parameters, Speech Technology.
Abstract: Coughing and shortness of breath are typical symptoms in people suffering from COPD, asthma, and COVID-
19 conditions. Separate studies have shown that coughing and respiratory health parameters, respectively, can
be sensed from a conversational speech recording using deep learning techniques. This paper looks into joint
sensing of coughing events and the breathing pattern during natural speech. We introduce an algorithm and
demonstrate its performance in realistic recordings. We observed sensitivity of 92.4% and 91.6% for cough
detection and breath event detection, respectively.
Clinical Relevance: Joint sensing of coughing events and respiratory parameters gives a more holistic picture
of the respiratory health of a patient which can be very useful for future telehealth services.
1 INTRODUCTION
The importance of respiratory sensing and cough
monitoring needs little justification, especially in
home monitoring of patients suffering from
respiratory conditions. The COVID-19 pandemic
demonstrated the necessity of remote digital health
assessment tools for telehealth services. This is
particularly pertinent for elderly and vulnerable
populations who already have a chronic disease. Post-
covid patients may suffer from respiratory symptoms
for several months after a severe form of COVID-19
disease and separate telehealth services are being
developed for these patients.
Speech is a good indicator of the pathological
condition of a person (Alireza A. Dibazar, et al.,
2002), especially for respiratory conditions like
COPD, asthma, and COVID-19. These conditions
significantly influence the breathing capacity and
cause vocal respiratory symptoms such as coughing
or wheezing.
We can hear when a person has breathing
difficulties or coughing, but the automatic detection
is a complex task. The breathing planning is complex
process based on linguistic and prosodic factors
(Marcin Włodarczak, et al., 2015) and the detection
of breathing events from continuous speech is
difficult.
We have demonstrated recently that it is possible
to use neural networks to estimate the breathing
parameters from a speech audio signal (Venkata
Srikanth Nallanthighal, et al., 2019; V. S.
Nallanthighal, et al., 2020). Neural networks have
also been used successfully for the detection of cough
sounds from non-speech recordings (A. C. den
Brinker, et al., 2021; Justice Amoh and Kofi Odame,
2016; Yusuf A Amrulloh, et al., 2015; Hui-Hui
Wang, et al., 2015). However, the current authors are
not aware of an earlier studies on the simultaneous
detection of coughs and respiratory behavior in
conversational speech recordings. Obviously,
speaking, breathing, and coughing are all functions of
the lungs, and tightly interlinked, which makes the
simultaneous sensing a challenging problem. One of
the key questions is related to the causal relations and
independence of different sensing targets. The results
of this paper seem to indicate that holistic sensing of
different aspects of respiratory health from a free
speech data is possible using modern machine
learning techniques.
2 BACKGROUND
The current research is related to the development of
acoustic sensing technology for telehealth call
services especially for patients with respiratory
Nallanthighal, V., Harm, A., Rietman, R. and Strik, H.
Detection of Coughing and Respiratory Sensing in Conversational Speech.
DOI: 10.5220/0010709700003123
In Proceedings of the 15th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2022) - Volume 5: HEALTHINF, pages 289-295
ISBN: 978-989-758-552-4; ISSN: 2184-4305
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
289

symptoms. In this scenario a nurse, or an automated
agent, has therapeutic conversations with the patient,
collects information, and answers questions about the
care or the symptoms. Breathing monitoring from
telehealth customers’ speech conversations over
multiple calls would give us the historical data of
breathing parameters and help us compare and
understand a person’s pathological condition,
decline, or improvement over time and early
detection of a condition.
The breathing, speech, and coughing, are all
functions closely related to the lungs, and influenced
by the condition of the respiratory system. Based on
physiological considerations, cough sounds are often
considered as consisting of four different phases :
inspiratory, contractive, compressive, and expulsive.
The inspiratory phase is initiated by breathing in and
is terminated by the closure of the glottis. In the
contractive phase, groups of respiratory muscles
contract, leading to a marked elevation of alveolar,
pleural, and subglottic airway pressures. In the
expulsive phase, the glottis opens quickly followed
by rapid exhalation of air under a large pressure
gradient.The rapid movement of air expelled from the
lung generates the cough sounds with contributions
coming from different areas of the respiratory system.
The mechanism of cough sound production shares
some similarities to that of speech production. The
current authors are not aware of a previous work
where the goal is simultaneous sensing of respiratory
parameters such as respiratory rate and coughing
activity and intensity from a conversational
recording.
In this paper we study joint detection of cough
events and sensing of respiratory health parameters,
such as breathing rate and tidal volume, from a
conversational speech recording. We give an
overview of the algorithms for cough detection and
respiratory signal estimation and compare those to the
corresponding state-of-the-art systems. Next, we
evaluate their performance in a speech data where the
goal is a joint sensing of the respiratory parameters,
and detection of coughing during speech. The first
results presented in this paper show that the two
models can work relatively independently. In the
discussion, we propose that joint sensing of breathing,
speaking, and coughing can be potentially modeled
using a holistic cardio-pulmonary speech model that
also takes the linguistic context into account.
Chronic obstructive pulmonary disease (COPD)
is a progressive respiratory disease characterized by
chronic inflammation of the lung airways which
results in airflow limitation. This results in frequent
shortness of breath (SOB) and coughing. SOB can be
detected from one’s speech (Sander Boelders, et al.,
2020). Coughing is a prominent indicator of several
problems such as COPD, and it is also the main
reason for why patients seek medical advice.
Frequent COPD exacerbations are associated with a
high mortality and heavy use of healthcare resources.
COPD patients with chronic cough and shortness of
breath may represent a target population for whom
specific respiratory sensing and cough monitoring
strategies should be developed.
3 METHODS
3.1 Respiratory Sensing from Speech
Both the rib cage and the abdomen can be used to
modulate alveolar pressure and airflow during
speech. Some speakers exhibit the stronger use of rib
cage over abdominal contributions, and some
speakers show a relatively equal contribution from
both the rib cage and abdomen (Thomas J. Hixon, et
al., 1976). When a known air volume is inhaled and
measured with a spirometer, a volume-motion
relationship can be established as the sum of the
abdominal and rib cage displacements (K. Konno and
J. Mead, 1967).
The Philips read speech database was collected at
Philips Research, Eindhoven, The Netherlands in
2019, with the approval of the Internal Committee
Biomedical Experiments (ICBE) of Philips Research.
The data was collected using the following setup: two
respiratory elastic transducer belts over the ribcage
under the armpits and around the abdomen at the
umbilicus level to measure the changes in the cross-
sectional area of ribcage and abdomen at the sample
rate of 2kHz. These belts work on the principle of
respiratory inductance plethysmography (RIP).
Earthworks microphone M23 is used for recording
high-quality speech at 48kHz. The microphone is
placed at a distance of one meter from the speaker,
and the data collection is conducted in a specialized
audio room for noise-free and echo-free recordings.
40 healthy subjects with no respiratory conditions(18
female and 22 male with age group ranging from 21
to 40 years old) are asked to read ”The Rainbow
Paragraph”, a widely used phonetically balanced
paragraph (G. Fairbanks, 1960).
In our data collection two respiratory belts were
placed around the rib cage under the armpits and
around the abdomen at the level of the umbilicus,
respectively. These belts work on the principle of
respiratory inductance plethysmography (RIP). They
consist of a sinusoidal wire coil insulated in elastic.
HEALTHINF 2022 - 15th International Conference on Health Informatics
290
Dynamic stretching of the belts creates waveforms
due to change in self-inductance and oscillatory
frequency of the electronic signal and the electronics
convert this change in frequency to a digital
respiration waveform where the amplitude of the
waveform is proportional to the inspired breath
volume. Thus the sum of rib cage and abdomen
expansions measured by the respiratory belt
transducers is considered as the measure for the
breathing signal.
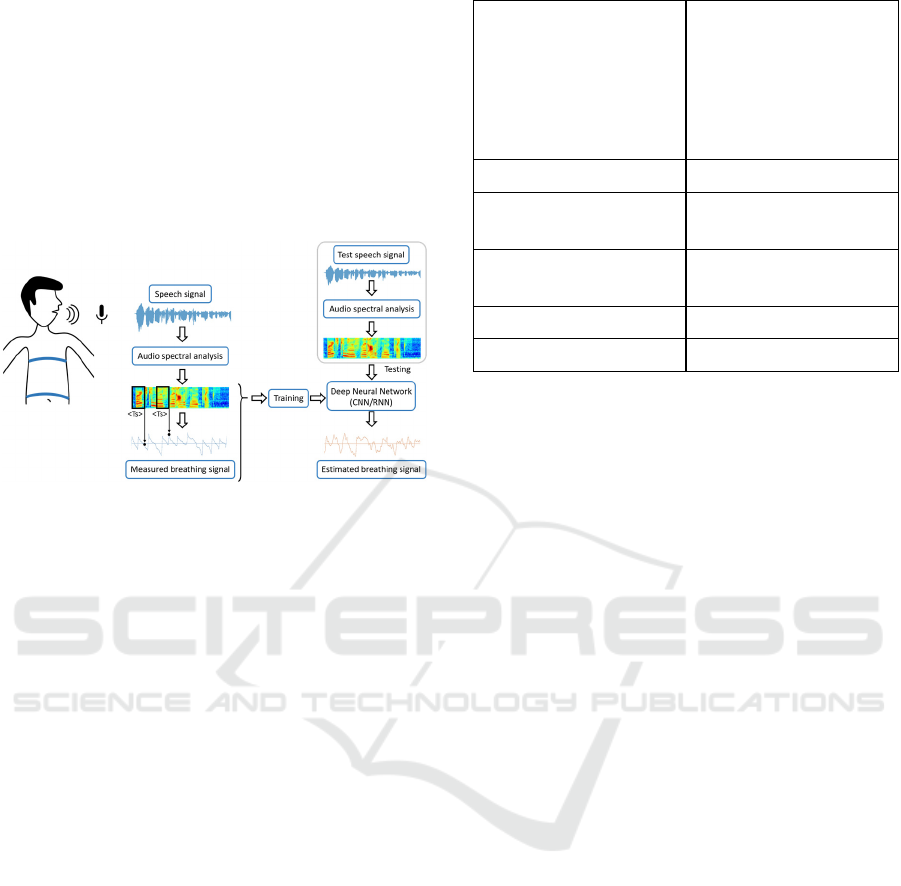
Figure 1: Schematic diagram for estimating respiratory
signal using Deep Neural Network Model based on spectral
features.
Estimating breathing signals from the speech
signal is a regression problem. The breathing signal is
a quasi-periodic signal whose characteristics are
dependent on the prosodic and linguistic content of
the speech signal. This information of speech can be
modeled using spectral features. Spectral features are
based on a time-frequency decomposition of the
speech signal. In this paper we use a linear
spectrogram computed using short-time Fourier
transform, and a nonlinear spectrogram with
logarithmic magnitude values on a Melfrequency
scale, i.e., log Mel spectrogram.
The spectrogram and log Mel spectrogram of a
speech signal of a fixed time window are mapped
with respiratory sensor value at the endpoint of the
time window with a stride of 10ms between windows
for Philips database to train the neural network
models as shown in Figure 1. These models will
estimate the respiratory sensor values of a speech
signal in real time to get the breathing pattern.
Using spectral features as an input representation
of speech signal, we implement convolutional neural
network (CNN) and Long short-term memory
recurrent neural network (RNNLSTM) models using
the PyTorch software framework (Adam Paszke,
2019). In the CNN model (Jürgen Schmidhuber,
2015), the data is fed into a network of two
convolutional layers with a single-channel and kernel
CNN Model RNN Model
Input: log Mel spectrogram Input: log Mel spectrogram
or spectrogram or spectrogram
m: frames in time window m: frames in time window
n : Mel filter banks n : Mel filter banks
Matrix X
i
(1 x m x n) Matrix X
i
(1 x m x n)
1 x conv3-1;s1
Maxpooling 3x3
LSTM model
1x conv5-1;s1
Maxpooling 3x3
Layers =2
3 Fully Connected layers Hidden size= 128
OUTPUT: sensor value OUTPUT: sensor value
Figure 2: Deep neural network configurations of the
spectral based methods for sensor value prediction.
size of 3 and 5 respectively for filtering operation to
extract local feature maps. Max pooling is deployed
to reduce the dimensionality of feature maps while
retaining the vital information. The rectified linear
unit activation function is applied to introduce non-
linearity into the feature extraction process for each
convolutional layer, as shown in Figure 2. Batch
normalisation is also applied on each convolution
layer. This is followed by 3 fully connected layers
with ReLU activation function. The Adam optimiser
(Diederik P. Kingma and Jimmy Ba, 2015) with a
weight decay of 0.001 is used as an optimization
algorithm.
In the RNN-LSTM model, the data is fed into a
network of two LSTM layers with 128 hidden units
and a learning rate of 0.001. The Adam optimizer is
used as an optimization algorithm to update network
weights iteratively based on training data (Diederik P.
Kingma and Jimmy Ba, 2015). These
hyperparameters for the network were chosen for
estimation after repeated experimentation.
As estimating breathing pattern from speech using
neural networks is a regression problem, we use the
following two metrics for evaluation and comparison:
correlation and mean squared error(MSE) of
estimated breathing signal and the actual respiratory
sensor signal. Also, we compare the breathing
parameters derived from the estimated and actual
breathing signals. The model that estimates breathing
signals with a higher correlation, lower MSE, and
comparable breathing parameters would be
considered best for our study.
Detection of Coughing and Respiratory Sensing in Conversational Speech
291
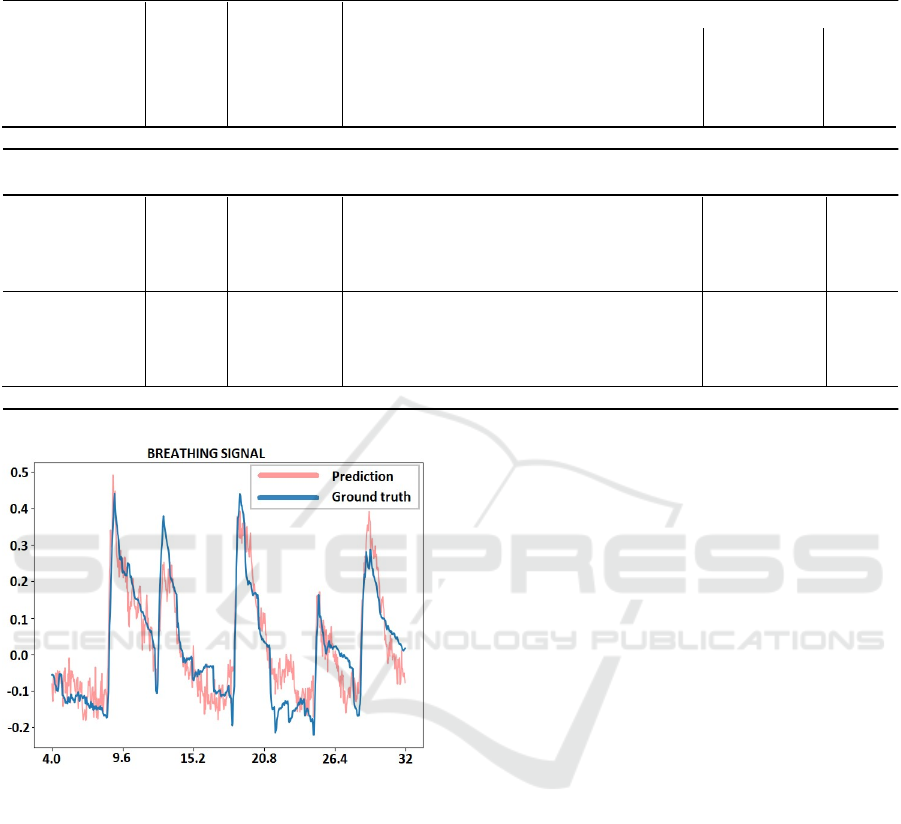
Table 1: Philips Database (read speech protocol): The r, MSE and breathing parameters for systems using spectral base
d
approach.
Breathing Parameters
Models
Loss
Function
r MSE
Breathing Rate
prediction true error
(breaths/min) (breaths/min) (%)
Breath Event
Sensitivity
Tidal
Volume
error
(%)
Spectral Based Approach
I/P: log Mel spec
O/P: sensor
Architecture:
RNN
MSE
BerHu
0.476
0.482
0.019
0.039
10.42
10.98
9.84
9.84
5.89%
11.58%
0.916
0.902
12.11%
16.24%
I/P: log Mel spec
O/P: sensor
Architecture:
CNN
MSE
BerHu
0.472
0.462
0.034
0.042
10.85
11.78
9.84
9.84
10.26%
19.71%
0.896
0.821
16.22%
18.84%
Figure 3: The predicted and ground truth for breathing
signal Table I presents the performance of the systems
trained and tested on the Philips database.
3.2 Cough Monitoring
Cough is an important clinical symptom in respiratory
diseases, yet there is not any gold standard to assess
it. The most common approach to addressing these
challenges is to find features of the acoustic signal
that offer good discrimination between coughs and
non-cough sounds. Barry et al,. used Linear
Predictive Coding and Mel-frequency Cepstral
Coefficients (MFCC) to model the sound of coughs
and used a Probabilistic Neural Network to classify
time windows as containing a cough or not (Samantha
J. Barry, et al., 2006). Other researchers have
explored other features based on adaptations of
speech recognition features (Thomas Drugman, et al.
2011) and custom-designed handcrafted features
(Eric C. Larson, et al., 2011). In this paper, we explore
advanced machine learning algorithms like XGBoost
models and deep learning algorithms for cough
detection.
The data of cough sounds is collected from a recent
trial of COPD patients in their home environment.
The data consist of one second audio snippets of
night-time recordings in the vicinity of COPD
patients, where the monitoring period ran over a
period of 90 days. Part of this data has been annotated
and is used in our study.
1) XGBoost Models:
In classical machine learning, a model is
trained on features that are extracted from the
signal. For each sound snippet, 12 MFCCs are
extracted around the peak of the transient.
Additionally, the sound levels just before and
after the peak are extracted, as well as the
number of acoustic transients in the 60 second
interval centered on the time of the recorded
snippet. An XGBoost (Tianqi Chen and Carlos
Guestrin, 2016) model was trained on the
features of the annotated snippets.
2) Deep Learning Models:
Convolutional and recurrent neural networks
are used for cough detection. In the CNN, the
input is a fixedsized image, a segment of the
logMel spectrogram, and the output is a single
HEALTHINF 2022 - 15th International Conference on Health Informatics
292

label. The RNN takes in a sequence of spectral
frames and outputs a sequence of labels.
The CNN architecture was inspired by the
popular LeNet-5 architecture (Yann LeCun, et
al., 2015) which yielded state-of-the-art
performance on the MNIST handwritten digits
dataset. Compared to other well-known
architectures such as the AlexNet, LeNet-5 is a
much smaller network and more suitable for
smaller datasets.
The RNN model consists of 6 layer encoder-
decoder architecture, which allows the
network to process and classify input
sequences of arbitrary length. The encoder is
made up of 3 layers: 2 bidirectional recurrent
layers with 128 and 64 units respectively and a
unidirectional layer with 32 recurrent units.
Our encoder is set up to process sequences of
up to a certain maximum length we set
depending on the experiment (see experiment
section below). All recurrent neurons in the
encoder are Gated Recurrent Units (GRU),
which can identify longterm dependencies in a
sequence of input data. The last layer of the
encoder outputs a fixed representation (the 32
activations) which is then used to initialize the
decoder. The decoder is a single recurrent
layer of 64 Long Short Term Memory (LSTM)
units, combined with an attention mechanism.
The attention mechanism enables the network
to focus on salient parts of the input features
and ultimately results in improved
classification performance. Currently, our
decoder is set up to output a single label for
each input sequence. Following the decoder,
we have a fully connected layer with 256
ReLU neurons. Finally, the classification layer
outputs a class label using the softmax
function.
Table 2: Comparison of cough detection models.
Models AUC scores standard
deviation
XGBoost Model 0.9040 0.0740
CNN (LeNe
t
-5) 0.9116 0.0576
RNN(seq2seq) 0.9141 0.0502
4 EXPERIMENTS ON JOINT
SENSING
The goal of joint sensing of respiration and cough
events is to verify if the models developed
independently for respiratory sensing and cough
detection can work together. The hypothesis to
support this is that the two models are trained on two
different datasets specific for respiratory sensing and
cough detection, respectively.
4.1 Joint Data Set
We collected a database of speech recordings with
coughs of 10 healthy volunteers(6 Male and 4
Female) who were asked to read ”The Rainbow
Paragraph”, a widely used phonetically balanced
paragraph (G. Fairbanks, 1960). The participants
were asked to voluntarily cough at random places
while reading the paragraph. Each recording is about
2 minutes long with at least five coughs. Cough
events and breathing events were annotated manually
by the authors for each of the ten subjects. We found
and manually annotated a total of 54 cough events and
103 breathing events for the ten recordings. This
database is used for testing our models on cough
monitoring and respiratory detection simultaneously.
4.2 Results
1) Performance of Respiratory Sensing: The pre-
trained deep learning model using RNN architecture
is used to compute the estimated respiratory signal for
each of the ten recordings. From these estimated
respiratory signals, respiratory breathing events are
identified using an Automatic Multiscale Peak
Detection Algorithm (AMPD) (Felix Scholkmann, et
al.,2012). These breath events computed from the
estimated respiratory signal are compared with the
manually annotated ground truth breath events, and
the results are formulated in Table III
2) Accuracy in Cough Detection: The RNN model
described in the previous section is used for cough
detection for each of the ten recordings. A total of 54
cough events are present in these ten recordings.
Actual cough events are compared against the
detected cough events to measure precision and
sensitivity and are reported in Table III.
Table 3: Joint detection of cough events and respiratory
events.
Modality Total
events
Precision Sensitivity
Cou
g
h detection 54 events 94,2% 92.4%
Breath event
detection
103 events 89.6% 91.6%
It is observed that joint sensing of cough and
respiratory events is plausible by using pre-trained
Detection of Coughing and Respiratory Sensing in Conversational Speech
293

models for individual tasks. We observed a precision
of 94.2% and sensitivity of 92.4% for the 54 cough
events and a precision of 89.6% and sensitivity of
91.6% for breath event detection.
5 CONCLUSIONS
An extensive study on methods for using speech as a
modality for respiratory sensing and cough
monitoring is presented in this paper. These strategies
are essential for patients suffering from respiratory
conditions, especially in remote monitoring services.
Our results evaluated on joint datasets of 10 healthy
volunteers conclude that joint sensing of coughs and
respiratory parameters is possible by training deep
learning models on separate datasets specific to
respiratory sensing and cough detection. However,
evaluation of this strategy on speech recordings of
patients suffering from respiratory conditions is
essential and is the future scope of our work.
ACKNOWLEDGMENT
This work was partially supported by the Horizon
H2020 Marie Skłodowska-Curie Actions Initial
Training Network
European Training Network project under grant
agreement No. 766287 (TAPAS) and Data Science
Department, Philips Research, Eindhoven.
REFERENCES
Alireza A. Dibazar, S. Narayanan, and Theodore W.
Berger, “Feature analysis for automatic detection of
pathological speech,” in Proceedings of the Second
Joint 24th Annual Conference and the Annual Fall
Meeting of the Biomedical Engineering Society,
Engineering in Medicine and Biology. IEEE, 2002, vol.
1, pp. 182–183.
Marcin Włodarczak, Mattias Heldner, and Jens Edlund,
“Breathing in conversation: An unwritten history,” in
Proceedings of the 2nd European and the 5th Nordic
Symposium on Multimodal Communication: 2015,
number 110 in Linkoping Electronic Conference
Proceedings,¨ pp. 107–112.
Venkata Srikanth Nallanthighal, Aki Harm¨ a, and Helmer
Strik, “Deep¨ Sensing of Breathing Signal During
Conversational Speech,” in Proc. Interspeech 2019,
2019, pp. 4110–4114.
V. S. Nallanthighal, A. Härmä, and H. Strik, “Speech
breathing estimation using deep learning methods,” in
ICASSP 2020 - 2020 IEEE International Conference on
Acoustics, Speech and Signal Processing (ICASSP),
2020, pp. 1140–1144.
A. C. den Brinker, M. Coman, O. Ouweltjes, M. G. Crooks,
S. Thackray-Nocera, and A. H. Morice, “Performance
requirements for cough classifiers in real-world
applications,” in 2020 28th European Signal
Processing Conference (EUSIPCO). IEEE, 2021, pp.
96–100.
Justice Amoh and Kofi Odame, “Deep neural networks for
identifying cough sounds,” IEEE transactions on
biomedical circuits and systems, vol. 10, no. 5, pp.
1003–1011, 2016.
Yusuf A. Amrulloh, Udantha R. Abeyratne, Vinayak
Swarnkar, Rina Triasih, and Amalia Setyati,
“Automatic cough segmentation from non-contact
sound recordings in pediatric wards,” Biomedical
Signal Processing and Control, vol. 21, pp. 126–136,
2015.
Hui-Hui Wang, Jia-Ming Liu, Mingyu You, and Guo-
Zheng Li, “Audio signals encoding for cough
classification using convolutional neural networks: A
comparative study,” in 2015 IEEE International
Conference on Bioinformatics and Biomedicine
(BIBM). IEEE, 2015, pp. 442–445.
Sander Boelders, Venkata Srikanth Nallanthighal, Vlado
Menkovski, and Aki Harm¨ a,¨ “Detection of mild
dyspnea from pairs of speech recordings,” in ICASSP
2020-2020 IEEE International Conference on
Acoustics, Speech and Signal Processing (ICASSP).
IEEE, 2020, pp. 4102–4106.
Thomas J. Hixon, Jere Mead, and Michael D. Goldman,
“Dynamics of the chest wall during speech production:
Function of the thorax, rib cage, diaphragm, and
abdomen,” Journal of speech and hearing research,
vol. 19, no. 2, pp. 297–356, 1976.
K. Konno and J. Mead, “Measurement of the separate
volume changes of rib cage and abdomen during
breathing,” Journal of Applied Physiology, vol. 22, no.
3, pp. 407–422, 1967, PMID: 4225383.
G. Fairbanks, “The rainbow passage,” Voice and
articulation drillbook, vol. 2, 1960.
Adam Paszke, Sam Gross, Francisco Massa, Adam Lerer,
James Bradbury, Gregory Chanan, Trevor Killeen,
Zeming Lin, Natalia
Gimelshein, Luca Antiga, Alban Desmaison, Andreas
Kopf, Edward Yang, Zachary DeVito, Martin Raison,
Alykhan Tejani, Sasank Chilamkurthy, Benoit Steiner,
Lu Fang, Junjie Bai, and Soumith Chintala, “Pytorch:
An imperative style, high-performance deep learning
library,” in
Advances in Neural Information Processing
Systems 32, H. Wallach, H. Larochelle, A.
Beygelzimer, F. d'Alche-Buc, E. Fox, and R. Garnett,´
Eds., pp. 8024–8035. Curran Associates, Inc., 2019.
Jurgen Schmidhuber, “Deep learning in neural networks:
An overview,Ӭ Neural Networks, vol. 61, pp. 85 Р117,
2015.
Diederik P. Kingma and Jimmy Ba, “Adam: A method for
stochastic optimization,” Computing Research
Repository (CoRR), vol. abs/1412.6980, 2015.
HEALTHINF 2022 - 15th International Conference on Health Informatics
294

Samantha J. Barry, Adrie D. Dane, Alyn H Morice, and
Anthony D Walmsley, “The automatic recognition and
counting of cough,” Cough, vol. 2, no. 1, pp. 1–9, 2006.
Thomas Drugman, Jerome Urbain, and Thierry Dutoit,
“Assessment of audio features for automatic cough
detection,” in 2011 19th European Signal Processing
Conference. IEEE, 2011, pp. 1289–1293.
Eric C. Larson, TienJui Lee, Sean Liu, Margaret Rosenfeld,
and Shwetak N. Patel, “Accurate and privacy
preserving cough sensing using a low-cost
microphone,” in Proceedings of the 13th international
conference on Ubiquitous computing, 2011, pp. 375–
384.
Tianqi Chen and Carlos Guestrin, “XGBoost: A scalable
tree boosting system,” in Proceedings of the 22nd ACM
SIGKDD International Conference on Knowledge
Discovery and Data Mining, New York, NY, USA,
2016, KDD ’16, pp. 785–794, ACM.
Yann LeCun et al., “Lenet-5, convolutional neural
networks,” URL: http://yann. lecun. com/exdb/lenet,
vol. 20, no. 5, pp. 14, 2015.
Felix Scholkmann, Jens Boss, and Martin Wolf, “An
efficient algorithm for automatic peak detection in
noisy periodic and quasi-periodic signals,” Algorithms,
vol. 5, no. 4, pp. 588–603, 2012.
Detection of Coughing and Respiratory Sensing in Conversational Speech
295
