
An Online Balance Training Application using Pose Estimation and
Augmented Reality
Amirhossein Etaat
1
, Negar Haghbin
1 a
and Marta Kersten-Oertel
1,2 b
1
Gina Cody School of Computer Science and Engineering, Concordia University, Montr
`
eal, Canada
2
PERFORM Centre, Concordia University, Montr
´
eal, Canada
Keywords:
Healthy Aging, Rehabilitation, Pose Estimation, Web Applications, Balance Training, Augmented Reality.
Abstract:
The evolution of digitally connected devices and artificial intelligence has opened the door for novel health
and fitness applications that can be used by individuals at a time and in an environment convenient to them.
The purpose of our research was to develop a platform that requires no additional hardware to provide an
online home balance training program. Balance exercises are often prescribed for healthy aging to keep the
body active, improve balance and coordination, and prevent falls and injuries, as well as, for those doing
rehabilitation after injuries or diseases such as stroke. We developed a simple web application (BaART:
Balance Augmented Reality Trainer) that uses PoseNet to determine a user’s location and pose for balance
exercises. Furthermore, we looked at how augmented reality, and specifically adding a virtual chair, might
impact a user’s sense of balance. In a study of 20 participants with and without balance disorders, we found
that the developed system was easy to use, however, we also found that the virtual object (i.e. chair) was not
used by most people. Furthermore, those with balance issues felt they required a real chair for balance and
some even felt that the virtual object was distracting from the exercise. In the future, we will explore other
uses of augmented reality, such as feedback on exercise quality, gaming features, and a virtual avatar trainer.
1 INTRODUCTION
As smart mobile phones and internet connections
become more accessible than ever, mobile health
(mHealth) applications are becoming ever more pop-
ular with many seeking to take their health into their
own hands within their own environments. This has
led to growing availability of web and mobile appli-
cations for rehabilitation, virtual coaches for training
and exercise, online doctor visits, and mental health,
meditation, and fitness applications.
In this paper, we focus specifically on rehabilita-
tion and balance exercises. Balance exercises which
work the core muscles, lower back, and legs are often
prescribed for healthy aging to keep the body active,
improve balance and coordination, and prevent falls
and injuries. They are also used in rehabilitation after
injuries or diseases such as stroke. New sensing (e.g.
wearables) and communication technologies (e.g. in-
ternet of things) are positively influencing the expan-
sion of training and rehabilitation programs outside
a
https://orcid.org/0000-0002-9598-9936
b
https://orcid.org/0000-0002-9492-8402
of standard healthcare facilities. It is now feasible to
do guided online exercises ensuring that they are done
correctly and even track a person’s progress over time
in the comfort of one’s own environment without di-
rect contact with a physiotherapist or trainer. This can
be done using different motion-tracking devices such
as wearable sensors, depth cameras and most recently
using pose estimation from simple web camera feeds.
Pose estimation is the task of using machine learning
models to estimate the pose of a person from an im-
age or a video by determining the spatial location of
keypoints (i.e. knee, elbow, nose, etc). Pose estima-
tion is beginning to be widely used in training robots,
motion tracking for game consoles, augmented real-
ity, animation, and health and fitness applications.
Gamification, i.e. the introduction of game ele-
ments to traditionally non-gaming situations, has also
proved to be an important aspect of mhealth applica-
tions, which can encourage and motivate users to not
only comply with their exercise regimes but also to
help them to enjoy doing so (Haghbin and Kersten-
Oertel, 2021). Augmented reality (combining virtual
and real elements) can also be used both for aiding
users to better understand exercises and the proper
168
Etaat, A., Haghbin, N. and Kersten-Oertel, M.
An Online Balance Training Application using Pose Estimation and Augmented Reality.
DOI: 10.5220/0010973800003188
In Proceedings of the 8th International Conference on Information and Communication Technologies for Ageing Well and e-Health (ICT4AWE 2022), pages 168-176
ISBN: 978-989-758-566-1; ISSN: 2184-4984
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

way of doing them and/or for adding gaming elements
to make exercising more enjoyable.
In this paper, we focus on delivering balance train-
ing exercises into the comfort of a user’s own home
using simple and low-cost technology (only a web-
cam and connected digital device are needed). Fur-
thermore, we explore the use of augmented reality
elements, i.e. adding a virtual chair for balance, to
see if this can aid users to perform balance exercises.
In order to study these questions, we developed a
balance training exercise prototype system, “Balance
Augmented Reality Trainer” (BaART) and tested it
with 20 subjects to determine the impact of the virtual
elements and in general the ease of use of the system.
2 RELATED WORK
2.1 Pose Estimation Health Applications
Encouraging people to exercise by exploiting tech-
nology at home can be a strategy that may be cost-
effective, particularly if consumer-level equipment is
used. A number of research groups have looked at us-
ing simple applications with webcams and using pose
estimation algorithms to determine the location of the
user’s joints in order to help guide and monitor exer-
cises. Pose estimation specifically refers to computer
vision techniques that can be used to detect human
figures in images and videos. By taking a processed
camera image as the input, pose estimation models
outputs information about the keypoints (e.g. elbow,
nose, knee, etc.) which can then further be used to
determine the pose of a person.
Moreira et al. (Moreira et al., 2020a) systemati-
cally reviewed mobile applications proposed for ana-
lyzing human posture. Their results showed that the
use of human pose estimation on mobile applications
is reliable, and can assist medical clinics, and physio-
therapists, especially in the case of evaluating physi-
cal treatments. Moreira et al. (Moreira et al., 2020b)
also proposed a prototype application using PoseNet
(a real-time pose detection library) and the Tensor-
Flow library for automatic identification of Anatom-
ical and Segment Points (ASPs). Their results show
that PoseNet can be used to develop applications con-
cerning the physical assessment process and diag-
nosis of disorders related to postural and movement
changes. Herrera et al. (Herrera et al., 2020) devel-
oped a web application, using Posenet and Tensor-
Flow, for sedentary workers to help them take active
pauses (i.e. pausing work to do exercises) in order
to reduce the risk of job-related muscular and skele-
tal injuries and diseases. The application accurately
determined the position of the user and whether they
were doing the exercise correctly.
2.2 Balance Training
A number of previous research studies have employed
various technologies to help aging adults to train bal-
ance, with an aim to maintain health and reduce the
likely hood of falls (Jorgensen et al., 2013). Mosta-
jeran et al. (Mostajeran et al., 2019) presented an ap-
plication for balance training at home using the Mi-
crosoft Kinect Sensor V2. The application has a vir-
tual coach who gives balance training instructions and
demonstrated the exercises. The authors found that
adults have a more positive reaction towards using
a virtual coach for balance training compared to tra-
ditional health care approaches. In a similar work,
Kouris et al. (Kouris et al., 2018) proposed a system
that uses a virtual reality avatar and wearable sensors
for physiotherapy balance exercises. The wearable
sensors can monitor user activity and determine the
correctness of the balance exercises in real-time. Von-
stad et al. (Vonstad et al., 2020) developed a 2D cus-
tom balance training exergame (i.e. a type of exercise
that mixes exercise and video games) using a deep
learning based pose estimation system to detect hu-
man body parts and estimate three-dimensional (3D)
body positions. In their work, they compared three
systems: a Microsoft Kinect Sensor V2, a marker-
based three-dimensional motion capturing system and
a deep learning system using a digital camera. In
a study where participants played the balance ex-
ergame, the deep learning method had similar perfor-
mance to both the Kinect and the marker-based sys-
tem, demonstrating the feasibility of using less com-
plex hardware and sensors for these types of applica-
tions.
Ogonowski et al. (Ogonowski et al., 2016) devel-
oped a system that used individualized physical fit-
ness training, gamification and wearable sensors with
a Microsoft Kinect and simple TV. Their work illus-
trated the possibility of incorporating such systems
into the daily life of older adults. Hardy et al. (Hardy
et al., 2013) also developed an exergame to motivate
older adults to do balance exercises and gain training
based on the adaptation and exergame analysis. Their
findings suggest that elderly individuals accept mul-
timedia training and the adaptability notion improves
the system’s accessibility.
Smartphones are also beginning to be tested for
use for balance, rehabilitation and physiotherapy ex-
ercises. For example, Androutsou et al. (Androut-
sou et al., 2020) proposed a smartphone application
for patients with balance disorders that enables users
An Online Balance Training Application using Pose Estimation and Augmented Reality
169

to self-evaluate their activity and progress, communi-
cate with others using the system, and get real-time
feedback about their training, activities and progress
over time.
2.3 Augmented Reality in mHealth
A number of researchers have explored the use of
augmented reality in the context of fitness and reha-
bilitation applications and specifically the use of vir-
tual coaches or trainers (Tsiourti et al., 2014). Virtual
coaches have been explored to help clinicians moni-
tor the use of medications and seniors’ adherence to
specific guidelines for medication use (F
´
elix et al.,
2019) or to keep the elderly physically active (Bick-
more et al., 2009; Albaina et al., 2009). For example,
Felberbaum et al. (Felberbaum et al., 2018) explored
aspects of an AR-based virtual coach that would im-
prove older adults’ mobility. Features of such a virtual
coach would include virtual friends to walk with, hav-
ing interactive guidance to help define and reach goals
and online monitoring to determine risks such as falls.
Bickmore et al. (Bickmore et al., 2009) demonstrated
that the combination of a virtual coach and pedome-
ter can increase the amount of walking among older
adults.
Virtual training assistants or coaches do not nec-
essarily have to take on the form of a human avatar.
Albaina et al. (Albaina et al., 2009) proposed an ani-
mated flower that is used as a virtual trainer to boost
the motivation of individuals to walk. Their study
found that elderly users appreciated the flower vir-
tual trainer and had a positive tendency to use it over
a longer period of time. The results of their studies
also demonstrated that the virtual flower trainer was
effective in boosting the acceptance of such a system
among older adults, despite its uncommon form.
Other studies have incorporated AR technology
into the daily lives of older adults. Ku et al. (Ku et al.,
2019) used the 3D-ARS (3D interactive augmented
reality) system to determine its impact on people with
balance disorders. A randomized controlled study
with 36 people who could walk on their own and
could stand on one leg was done to assess the effect of
the AR technology. In comparing the control group,
who did a conventional physical fitness program three
times a week for 1 month, to the experimental group,
who used 3D-ARS training three times a week for 4
weeks, they found that although both groups experi-
enced improvements those who used of 3D-ARS had
better results in terms of stability index, weight distri-
bution index, fall risk index, and Fourier transforma-
tions index of posturography. Roy et al. (Roy et al.,
2017) developed a low-cost AR system using the Mi-
crosoft Kinect. The system guides users to perform
stability training and even calculates a real-time sta-
bility score.
3 SYSTEM DESCRIPTION
Using intervention and assessment tools at home can
considerably decrease the risk of falls and enhance
one’s quality of life through increased mobility and
in turn healthy aging (Society et al., 2001). Balance
training exercises and therapies are commonly used
to improve both balance and gait conditions. Accord-
ing to the American Geriatrics Society (Panel on Pre-
vention of Falls in Older Persons, 2011) a proper and
standard balance exercise plan can play a vital role
in health and rehabilitation. However, studies have
found that many patients and users do not do physio-
therapy exercises or training that can help or prevent
ailments due to a lack of motivation, time and/or the
high cost of physiotherapy, gyms, and hiring personal
trainers (Argent et al., 2018). Building on the previ-
ous works described above, our goal was to develop
a prototype system that requires no specialized equip-
ment but rather can be used in the comfort of one’s
desired environment by simply clicking on a url on
a computer, mobile phone, tablet, Smart TV or other
connected device. We also aimed to make the system
easy to use by providing a simple interface that in-
cludes voice commands and instructional videos. Our
developed home-based rehabilitation online app uses
(1) pose estimation to determine the users pose and
count the number or repetitions of a given exercise
and (2) explores the ability of augmented reality to
help with balance exercises. The motivation for the
latter, was to determine if a stationary object added
via a virtual object, which would provide a visual
static reference point, can improve balance. Although
this is the case for walking or balancing in the real
world it is unclear if virtual objects have the same im-
pact.
3.1 PoseNet
Our prototype uses PoseNet (Papandreou et al.,
2018), a library built on top of TensorFlow, which is
an open-source machine learning platform that pro-
vides an ecosystem of tools for developing machine
learning applications. PoseNet is trained in the Mo-
bileNet Architecture (a convolutional neural network
(CNN) developed by Google and trained on Ima-
geNet) and has pre-trained models that detect user
gestures and poses from given images. An advantage
of PoseNet in comparison to other API-dependent li-
ICT4AWE 2022 - 8th International Conference on Information and Communication Technologies for Ageing Well and e-Health
170

Figure 1: The user opens the application on a browser on any connected digital device. The web browser fetches data from
the server (written in HTML, CSS, JavaScript codes including Posenet Library and P5js library). The keypoints are detected
using the PoseNet model. The web application processes the captured inputs to determine exercises correctness and counts
repetitions, as well as, displays the AR object in the correct position relative to the user.
braries for pose estimation is that the pre-trained mod-
els run in a browser thus private data (i.e. images and
video stream from webcam) are protected and not sent
to a server for processing. Furthermore, anyone with a
webcam equipped desktop or TV, tablet or phone can
use PoseNet within their web browser. Taking advan-
tage of PoseNet allowed us to keep the system sim-
ple and highly accessible, without the need of devices
such as Kinect, wearables or motion capture systems
that can add complexity and may have high installa-
tion and preparation costs.
3.2 BaART: Balance AR Trainer
The BaART user interface was developed using
Javascript, HTML and CSS and PoseNet and Ten-
sorFlow’s models were used to recognize and esti-
mate the human poses. Pose estimation was specifi-
cally used to count the number of repetitions that were
done by the end user and check if the exercise has
been done correctly. We also used p5.Speech (an ex-
tension of p5.js which is an open-source JavaScript
library) for implementing speech-to-text and voice
commands.
The application pipeline is shown in Figure 1. As
mentioned above, the application uses a simple web-
cam without any further specialized equipment. After
opening the application via the provided URL on a
computer, laptop, or mobile device, RGBA input is
captured from the web camera and the user’s pose is
estimated via PoseNet. After successful keypoint de-
tection, the exercise routine begins. The keypoint data
(e.g. knee, ankles, hips, shoulders, eyes, etc.) is used
to determine the location of the user to both place the
virtual object and determine if an exercise is being
done. While exercises are being performed, the key-
points and movements are tracked so that the system
can evaluate if an exercise is being executed correctly
and the number of repetitions the user has done. Re-
sults are displayed to the user in real-time through the
interface, which shows the count and or repetitions
(either number of seconds or repetitions successfully
completed). The user can interact with the applica-
tion using either voice commands: “next exercises”,
“re-do”, “refresh” or “previous” or with a mouse on a
computer or gestures on a mobile device.
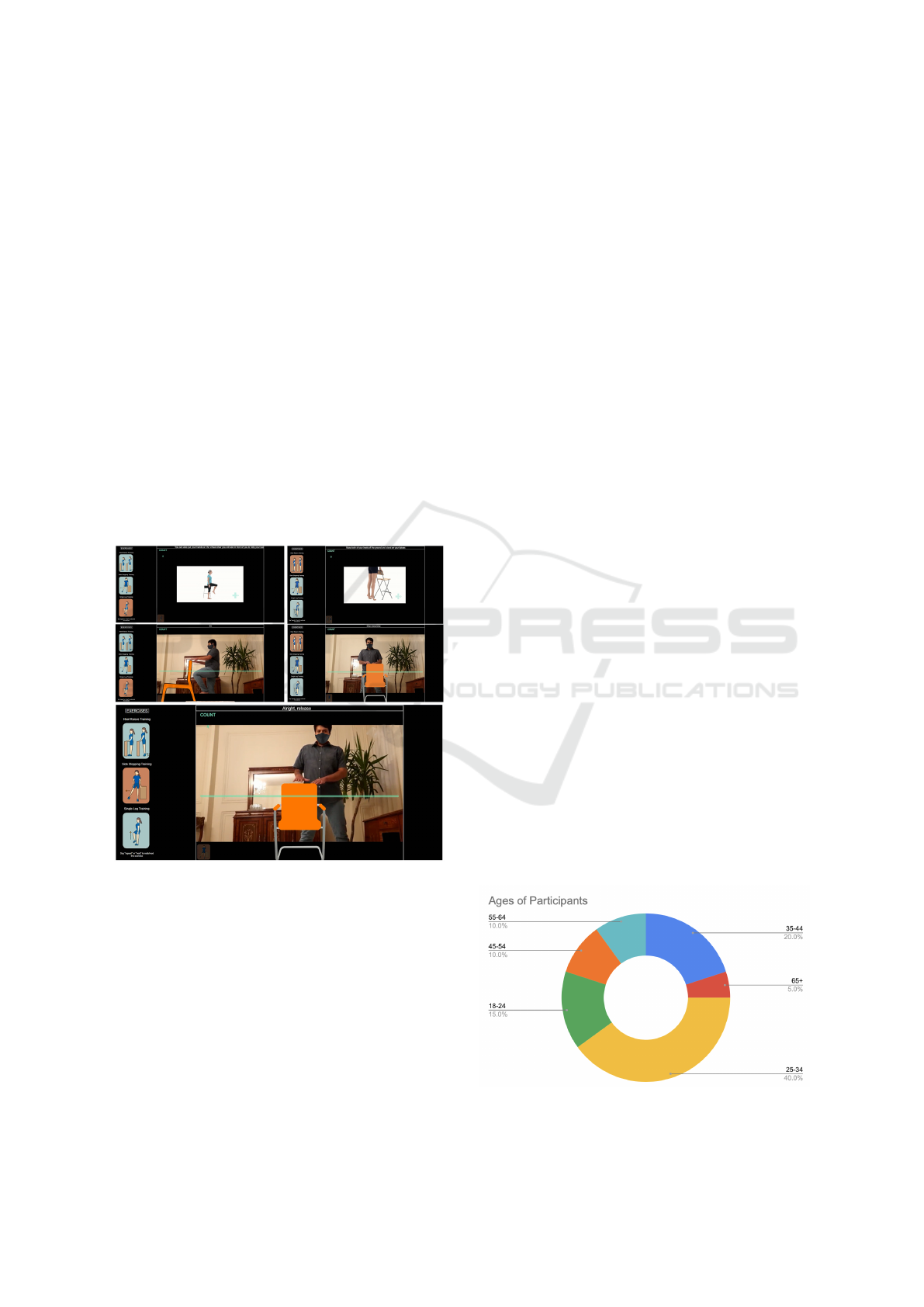
3.2.1 Exercises
For the first prototype of our system we selected three
exercises that improve balance and prevent falls based
on the clinical guidelines and recommendations of
the National Institute of Clinical Excellence (NICE)
and the joint American and British Geriatric Society
(ABGS) for the prevention and assessment of falls
in older people (National Institute for Health and
Care Excellence (NICE), 2013; Panel on Prevention
of Falls in Older Persons, 2011). Specifically, we
chose: heel raises, side stepping and single leg stand-
ing exercises (see Figure 2).
Tyagi et al. (Tyagi et al., 2018) studied the adop-
tion of technology-based telerehabilitation (TR) and
found that although younger users preferred TR, older
ones preferred daily visits to the rehabilitation center.
As in person visits are not always feasible particu-
larly for daily visits (or during a global pandemic),
Tyagi et al. recommended using videos in TR pro-
grams for older patients. Thus for each of the exer-
cises in the BaART application, an instructional video
(taken from www.Physitrack.com) is first shown to
explain how to do the exercise. After the video, the
user then does the given exercise following along with
both verbal and onscreen written instructions. As well
as giving instructions, the voice of the “trainer” tries
to motivate the user with encouraging statements and
counts the repetitions the user has done. We briefly
describe
Heel Raises: For heel raises, the keypoint informa-
tion is used to track the position of the hips of the
user while standing and uses the raising and lower-
ing of the hips to determine the number of repetitions.
Often times a chair is used for extra balance in heel
An Online Balance Training Application using Pose Estimation and Augmented Reality
171
raise exercises, thus we use a virtual chair to study if
“resting” one’s hands on a virtual chair can invoke a
sense of balance. The virtual chair is placed in front of
the determined location of the user. During the exer-
cise, the user raises both of their heels off the ground
to stand on their tiptoes. The user raises their heels
10 times, each time the application says “raise your
heels”, and then slowly lowers their heels back to the
floor when the application says “release”.
Side Step: For side stepping, the keypoint informa-
tion of the hips and shoulders are used to ensure the
user is stepping to the side correctly and to count the
repetitions. Again, a virtual chair is shown in front
of the user so that the user can “rest” their hands and
focus on this static point for better balance. This ex-
ercise starts with the feet together and knees slightly
bent, the user then moves one foot to the side and then
back to join the other foot. The instructions given are
“step right” to take a full right step and then “release”
to step back to the centre and bring the feet back to-
gether. The exercise is repeated 10 times.
Figure 2: The instructional videos demonstrating the three
exercises and user doing the exercises with the virtual chair.
The green line represents the position of the hips.
Single Leg Standing: For this exercise, the most
challenging of the three, keypoint information is used
to determine how high the leg is raised relative to the
distance to the pelvis. For this specific exercise, the
user is asked to rotate the body by 90 degrees to the
right or left in order to be able to best detect the knees.
The user is then instructed to stand upright with their
feet together, and try to slowly lift their foot off the
ground so their thigh is perpendicular to the floor. The
virtual chair is provided and the user is instructed to
do single leg standing for 15 seconds for the left and
then right leg.
3.2.2 User Interface
A simple user interface (UI) was developed so that
users of all ages can easily interact with BaART.
For instance, verbal communication and images were
used to convey information to the user. For those with
hearing problems, the words and sentences are tran-
scribed and displayed at the top of the interface. Also,
we tried to encourage and motivate the user after each
correct set using motivational and prompting words
and phrases, e.g. “good job!”, similar to a real trainer.
4 BaART EVALUATION
The BaART application was evaluated with 20 partic-
ipants aged 18 to 73 with 14 males and 6 females (see
Figure 3). Participants used the application online at
their convenience. Those who agreed to participate
were first sent a consent form, a description of the ap-
plication, instructions on how to use the BaART ap-
plication and a link to the application that they could
run on the device of their choice at their convenience.
4.1 Questionnaire
After the study, participants filled out a questionnaire
with both background questions and questions about
their experience with the application. Note that the
pre-test and post-test questionnaires were combined
to facilitate navigation between instructions, applica-
tion and questionnaires. The summary of the analy-
sis of the questionnaire are presented in the following
sections.
4.1.1 Technology Use
To determine comfort with new technologies, partic-
ipants were questioned on how they felt about their
Figure 3: The BaART application was evaluated with 20
participants aged 18 to 73 with 14 males and 6 females.
ICT4AWE 2022 - 8th International Conference on Information and Communication Technologies for Ageing Well and e-Health
172

practical knowledge of technology, and how often
they used a smartphone, tablet, or computer. The ma-
jority of participants (75%) use some form of digital
device daily, whereas 25% use a device only weekly.
In terms of their practical knowledge of technology,
which was answered on a scale from 1 (I don’t know
anything about technology) to 5 (I’m very technolog-
ically savvy), the majority of participants rated their
knowledge as 4 or 5, thus our sample participants
were technologically savvy.
We also asked how keen the participants are on
trying out new technologies from 1 (Not at all) and 5
(Yes I’m usually very keen) and found that 35% were
very keen, 40% were quite keen, 10% were neither
keen or not keen and 15% were not keen. Lastly,
we asked participants about the degree to which it
was easy and simple for them to use new technolo-
gies such as mobile apps and found that the majority
find it either very easy or somewhat easy.
4.1.2 Sport and Health Activities
The second part of the questionnaire queried users
about health and fitness activities. Specifically, partic-
ipants were asked if they considered themselves phys-
ically active as well as how often they participated in
fitness activities such as sports, aerobics, training, etc.
In a range of 1 (Not at all physically active) to 5 (Yes
I’m very physically active), only 1 person (5%) con-
sidered themselves very active, 30% considered them-
selves somewhat active and 40% considered them-
selves neither very active or inactive. Lastly, 25%
of participants considered themselves somewhat inac-
tive. In terms of how often participants exercised 40%
said 1-2 times a week, 40% 3-4 times a week, and
20% answered that they hardly ever exercise. None
of our participants exercised 5-6 times per week or
everyday. In terms of users ideal location for exercis-
ing, 30% prefer exercising at home, 35% at the gym,
30% prefer exercising outside and 5% said they didn’t
have a preference.
We also questioned participants about the main
factors that lead them to exercise less frequently than
they would like to. Here participants could select mul-
tiple answers. Of our population, 95% (19 people)
answered “I don’t have time”, 6 answered “I forget to
exercise”, one person answered “I don’t like exercis-
ing”, one other said “I don’t feel I need to exercise”,
and one person answered that they did not exercise
because they did not have someone else to exercise
with.
We also asked participants about their use of on-
line exercise training (e.g. Apple Fit+, Wii, YouTube
online class) and found that most participants (70%)
had not previously done online fitness classes or ex-
ercises whereas as 30% had. Lastly, participants
were asked if they have ever done any rehabilita-
tion, physiotherapy or balance training. For reha-
bilitation and/or physiotherapy 20% had done this,
whereas 80% had not. For balance training which
included balance exercises within yoga and rehabil-
itation/physiotherapy routines, we had 25% who had
done balance training in yoga or uni-cycling routines
and 75% who previously had not done any balance
exercises and one person (5%) who was not sure.
4.1.3 Balance Disorders
As our application concerns balance exercises, we
queried the participants about their experience of
dizziness, falls and loss of balance. Specifically, we
asked if participants had experienced a loss of balance
or had a balance problem leading to falls or near falls
in the last six months. The majority of participants
(65%) did not have any balance problems. More than
one-third of participants reported that they suffered
from dizziness and loss of balance. Specifically, 10%
had experienced a fall and 20% had nearly fallen. One
person had experienced both a near fall and had fallen
in the last six months.
4.1.4 Ease of Use
Participants were asked to rate the application on a
scale of 1 (Hard to understand) to 5 (Easy to under-
stand), for the video instructions and auditory coach-
ing instructions. We found that 60% found the video
instructions easy to understand (rated with 5), 35%
found the video instructions somewhat easy to under-
stand and 5% found them neither hard or easy. For
the spoken instructions, 55% found them easy to un-
derstand, 40% found them somewhat easy to under-
stand and 5% found them difficult to understand. We
also asked if the subjects used the voice commands
(next, repeat, previous) while doing the study. Most
of the participants, 80% used voice commands, 15%
did not and one person (5%) answered maybe. Of
those that used the voice commands, 11.5% found
them very easy to use, 47% found them somewhat
easy to use, 11.5% found them difficult to use, and
30% found them very difficult to use.
In terms of the overall system ease of use 50%
of the participants found it very easy, 35% found it
somewhat easy to use, 10% found it neither hard or
easy and one participant (5%) found it difficult to use.
The majority (80%) tested the application on laptops,
15% tested on workstation computers and 5% (1 per-
son) used a mobile device.
An Online Balance Training Application using Pose Estimation and Augmented Reality
173

4.1.5 Augmented Reality
As one of our goals was to determine if augmented re-
ality (provided by virtual objects introduced into the
video images) could aid in improving a sense of bal-
ance, we specifically asked users about their impres-
sion of this. First users were asked if they tried using
the virtual chair for the different exercises, we found
that 60% of participants did use the virtual chair, 20%
did not, and 20% answered maybe. Of those that used
the virtual object, we asked if it gave them an impres-
sion of helping them with their balance as they per-
formed their exercises. On a scale of 1 (It didn’t help
at all) to 5 (It helped me to balance), we found that
21% found it did not help at all, 10.5% found it did
not help, 32% were not sure, 26% thought it helped
a little to balance and 10.5% found it helped them to
balance. Furthermore, we asked participants if they
had any comments about the use of the virtual objects
for exercises, most of the participants didn’t have any
issue with using virtual objects, but we received some
comments including “I do not know how to use a vir-
tual object to maintain my balance”, “The virtual ob-
jects didn’t improve my performance”, as well as, “It
did not help much and sometimes made me lose my
focus on the exercise itself just because I wanted to
keep my hands on it”.
4.1.6 System Usability Scale
Finally, we provided participants with a version of
the System Usability Scale (SUS) (Brooke, 1996).
The questionnaire has ten questions positive and neg-
ative questions relating to a system’s usability. The
questions are answered on a scale of 1 to 5, with
1 representing Strongly Disagree and 5 representing
Strongly Agree with the question’s statement. The
BaART application received a SUS score of 80. The
average SUS score is 68, and given that a SUS value
of 75 is considered good, and over 85 is excellent, our
system was rated very highly with participants find-
ing who found it easy to use, easy to learn, and felt
confident using it. The results of the individual SUS
questions are represented in Table 1.
4.1.7 Using BaART in the Longer Term
We asked participants to answer on a scale from 1
(very unlikely ) to 5 (very unlikely) if they would use
BaART if the prototype was extended with more exer-
cises and features. Thirty percent of participants were
not sure if they would use such a system, 20% percent
and 50% said they would very likely use it.
We also queried specifically if the participants felt
that such an application can motivate them to exer-
cise whenever they did not feel like it or were busy,
by sending notifications to their phone, on a scale of
1 (No would not help at all) to 5 (Yes it would very
much help). We found that 5% said it would not help
at all and another 5% said it would not help and 15%
said they were not sure. However, 35% thought it
would help and 40% thought it would help very much.
Lastly, we had an open question to gather the par-
ticipant’s overall opinions about the prototype system.
Some commented on the exercises, e.g. ”Increase ex-
ercises”, ”I think the second exercise which was step
siding could be replaced to be a more effective exer-
cise”. A few users had difficulties with some aspects
of the app such as their pose not being recognized al-
though they mentioned they were able to resolve the
issues by moving the camera or their position relative
to the camera but this made them rate the usability
lower. We also had the following comments in terms
of the platform in general: ”It was good for me be-
cause I’m 77 years old and it’s hard for me to go to the
gym. But I needed a real chair or someone to help me
with doing exercises.” and ”Since I am a housewife
and I am usually at home, I think it is a good idea if I
can do exercises at home with this app”. In general,
we found that it was are older participants, who tend
to spend more time at home, who were more excited
about using such a system.
5 DISCUSSION AND FUTURE
WORK
The results of our work suggest that online home ex-
ercise routines for balance training may be desirable
for some users, though it may not be the ideal plat-
form for all. Specifically, we were happy to see that
our older population was excited about such a plat-
form. Although our participant pool was very tech
savvy, surprisingly 70% had not used online training
applications before, but did rate the BaART applica-
tion as easy and convenient to use.
In terms of the augmented reality visualization, al-
though our sample population did not have a signif-
icant portion of users with balance disorders, those
that had them, believed that they would require a real
object to help them for balance rather than a virtual
object. Furthermore, only 60% used the virtual ob-
ject and one person even mentioned it was distracting
from the exercises. We believe this still may be an in-
teresting avenue of future research, however, it might
require a better synchronization between verbal in-
structions and the visualization. For example, asking
the users to imagine having their hands on a real chair
while they step to the side. In future work, we plan to
ICT4AWE 2022 - 8th International Conference on Information and Communication Technologies for Ageing Well and e-Health
174
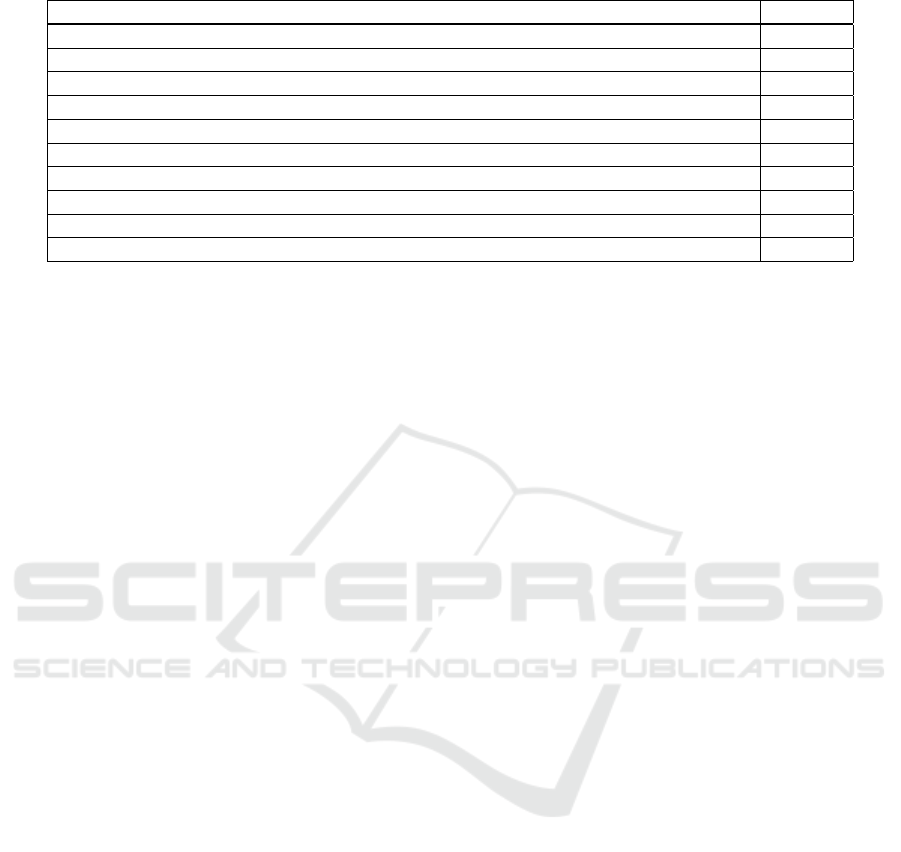
Table 1: System Usability Scale (SUS) average scores from 1 (strongly disagree) to 5 (strongly agree).
System Usability Scale Questions Average
I think that I would like to use this system frequently 3.65
I found the system unnecessarily complex 1.85
I thought the system was easy to use 4.3
I think that I would need the support of a technical person to be able to use this system 1.55
I found the various functions in this system were well integrated 4.55
I thought there was too much inconsistency in this system 1.6
I would imagine that most people would learn to use this system very quickly 4.25
I found the system very cumbersome to use 1.85
I felt very confident using the system 4.2
I needed to learn a lot of things before I could get going with this system 2.05
add more AR elements not necessarily for balancing
but to guide the exercises and add gaming elements.
One such example is an apple to pick from a tree when
raising on ones tiptoes. Adding gamification elements
such as this may make the application more engaging.
Furthermore, a virtual trainer or avatar that does the
exercises with you and adjusts their pace to the end
user may also be interesting.
Given this was a first prototype, we only had three
exercises and found users would be interested in hav-
ing more. In the future, we plan to extend the platform
to have more exercises and include other features as
suggested by the participants. Additional features in-
cluding: being able to either watch the tutorials again
or skip them, improving the voice commands which
some users had issues with (perhaps due to micro-
phone issues or accents) and into different languages
to accommodate non-native English speakers, enlarge
the text instructions, and send notifications to the user
to ensure they perform the exercises regularly.
Lastly, although we capture the pose and deter-
mine that the user is doing the exercise correctly in
order to count the repetition, the user does not receive
any visual or auditory feedback on the quality of the
exercise and how to improve it if they are doing it
wrong. In future work, we plan to relay this infor-
mation to the user. In general, collecting, analyzing,
and delivering performance-related data of users in
charts could motivate users further by showing them
the progress they have made.
As well as, the future directions described above it
will be important to do a longer term study with more
participants to look at not only how we can encourage
these healthy habits in the short term but change user
habits for sustained use.
6 CONCLUSION
In this paper, we describe a developed prototype for
doing balancing exercises at home based on the Na-
tional Institute of Clinical Excellence (NICE) guide-
lines for fall prevention and British Geriatric Soci-
ety (ABGS) set of clinical instructions to prevent and
evaluate older adults falls. We conducted a study with
20 users, both younger and older, and with and with-
out balance disorders. The results of our study indi-
cate that the participants liked the concept in general
and found the application easy to use. Furthermore,
they are interested in using this application, especially
if it were extended to have more exercises and fea-
tures such as notifications.
In terms of the augmented reality aspect, most
users found the virtual object did not help them to bal-
ance. Although this is the case, we posit that there are
additional possibilities to be explored for using AR in
such a system, including adding visual feedback on
the quality and correctness of the exercise, adding a
virtual coach, and adding gaming elements. The par-
ticipants of the study also felt that they do not exer-
cise as much as they like because it is time-consuming
and costly. Online fitness and health applications are
helping to mitigate these issues by allowing users to
have personal trainers to work with them whenever
and wherever they are.
REFERENCES
Albaina, I. M., Visser, T., Van Der Mast, C. A., and Vas-
tenburg, M. H. (2009). Flowie: A persuasive virtual
coach to motivate elderly individuals to walk. In In-
ternational Conference on Pervasive Computing Tech-
nologies for Healthcare, pages 1–7.
Androutsou, T., Kouris, I., Anastasiou, A., Pavlopoulos,
S., Mostajeran, F., Bamiou, D.-E., Genna, G. J.,
Costafreda, S. G., and Koutsouris, D. (2020). A
smartphone application designed to engage the elderly
in home-based rehabilitation. Frontiers in Digital
Health, 2.
Argent, R., Daly, A., Caulfield, B., et al. (2018). Patient in-
volvement with home-based exercise programs: can
An Online Balance Training Application using Pose Estimation and Augmented Reality
175

connected health interventions influence adherence?
JMIR mHealth and uHealth, 6(3):e8518.
Bickmore, T., Silliman, R., Nelson, K., Cheng, D., Winter,
M., Henault, L., and Paasche-Orlow, M. K. (2009). A
randomized controlled trial of an automated exercise
coach for older adults. Journal of the American Geri-
atrics Society.
Brooke, J. (1996). SUS: A “quick and dirty” usability scale.
Usability evaluation in industry, 189(3).
Felberbaum, Y., Lanir, J., and Weiss, P. L. (2018). Chal-
lenges and requirements for technology to support
mobility of older adults. In Extended Abstracts of the
2018 CHI Conference on Human Factors in Comput-
ing Systems, pages 1–6.
F
´
elix, I. B., Guerreiro, M. P., Cavaco, A., Cl
´
audio, A. P.,
Mendes, A., Balsa, J., Carmo, M. B., Pimenta, N.,
and Henriques, A. (2019). Development of a com-
plex intervention to improve adherence to antidiabetic
medication in older people using an anthropomorphic
virtual assistant software. Frontiers in Pharmacology,
10.
Haghbin, N. and Kersten-Oertel, M. (2021). Multimodal
cueing in gamified physiotherapy: A preliminary
study. In Proceedings of the 7th International Con-
ference on Information and Communication Technolo-
gies for Ageing Well and e-Health (ICT4AWE), pages
137–145. INSTICC, SciTePress.
Hardy, S., G
¨
obel, S., and Steinmetz, R. (2013). Adaptable
and personalized game-based training system for fall
prevention. In Proceedings of the 21st ACM interna-
tional conference on Multimedia, pages 431–432.
Herrera, F., Ni
˜
no, R., Montenegro-Mar
´
ın, C. E., Gaona-
Garc
´
ıa, P. A., de Mend
´
ıvil, I. S. M., and Crespo, R. G.
(2020). Computational method for monitoring pauses
exercises in office workers through a vision model.
Journal of Ambient Intelligence and Humanized Com-
puting, pages 1–9.
Jorgensen, M. G., Laessoe, U., Hendriksen, C., Nielsen, O.
B. F., and Aagaard, P. (2013). Efficacy of nintendo wii
training on mechanical leg muscle function and pos-
tural balance in community-dwelling older adults: a
randomized controlled trial. Journals of Gerontology
Series A: Biomedical Sciences and Medical Sciences,
68(7):845–852.
Kouris, I., Sarafidis, M., Androutsou, T., and Koutsouris,
D. (2018). Holobalance: an augmented reality virtual
trainer solution forbalance training and fall preven-
tion. In 2018 40th Annual International Conference
of the IEEE Engineering in Medicine and Biology So-
ciety (EMBC), pages 4233–4236. IEEE.
Ku, J., Kim, Y. J., Cho, S., Lim, T., Lee, H. S., and Kang,
Y. J. (2019). Three-dimensional augmented reality
system for balance and mobility rehabilitation in the
elderly: A randomized controlled trial. Cyberpsy-
chology, Behavior, and Social Networking, 22(2):132–
141.
Moreira, R., Teles, A., Fialho, R., Baluz, R., Santos, T. C.,
Goulart-Filho, R., Rocha, L., Silva, F. J., Gupta, N.,
Bastos, V. H., et al. (2020a). Mobile applications for
assessing human posture: A systematic literature re-
view. Electronics, 9(8):1196.
Moreira, R., Teles, A., Fialho, R., Dos Santos, T. C. P.,
Vasconcelos, S. S., de S
´
a, I. C., Bastos, V. H., Silva,
F., and Teixeira, S. (2020b). Can human posture
and range of motion be measured automatically by
smart mobile applications? Medical hypotheses,
142:109741.
Mostajeran, F., Katzakis, N., Ariza, O., Freiwald, J. P., and
Steinicke, F. (2019). Welcoming a holographic vir-
tual coach for balance training at home: two focus
groups with older adults. In 2019 IEEE Conference
on Virtual Reality and 3D User Interfaces (VR), pages
1465–1470. IEEE.
National Institute for Health and Care Excellence (NICE)
(2013). Falls: Assessment and prevention of falls in
older people.
Ogonowski, C., Aal, K., Vaziri, D., Rekowski, T. V., Ran-
dall, D., Schreiber, D., Wieching, R., and Wulf, V.
(2016). Ict-based fall prevention system for older
adults: qualitative results from a long-term field study.
ACM Transactions on Computer-Human Interaction
(TOCHI), 23(5):1–33.
Panel on Prevention of Falls in Older Persons (2011). Sum-
mary of the updated american geriatrics society/british
geriatrics society clinical practice guideline for pre-
vention of falls in older persons. Journal of the Amer-
ican Geriatrics Society, 59(1):148–157.
Papandreou, G., Zhu, T., Chen, L.-C., Gidaris, S., Tompson,
J., and Murphy, K. (2018). Personlab: Person pose es-
timation and instance segmentation with a bottom-up,
part-based, geometric embedding model. In Proceed-
ings of the European conference on computer vision
(ECCV), pages 269–286.
Roy, S., Mazumder, O., Chatterjee, D., Chakravarty, K., and
Sinha, A. (2017). Quantification of postural balance
using augmented reality based environment: A pilot
study. In 2017 IEEE SENSORS, pages 1–3. IEEE.
Society, A. G., Society, G., Of, A. A., and On Falls Preven-
tion, O. S. P. (2001). Guideline for the prevention of
falls in older persons. Journal of the American Geri-
atrics Society, 49(5):664–672.
Tsiourti, C., Joly, E., Wings, C., Moussa, M. B., and Wac,
K. (2014). Virtual assistive companions for older
adults: qualitative field study and design implications.
In Proceedings of the 8th International Conference
on Pervasive Computing Technologies for Healthcare,
pages 57–64.
Tyagi, S., Lim, D. S., Ho, W. H., Koh, Y. Q., Cai, V., Koh,
G. C., and Legido-Quigley, H. (2018). Acceptance of
tele-rehabilitation by stroke patients: perceived barri-
ers and facilitators. Archives of physical medicine and
rehabilitation, 99(12):2472–2477.
Vonstad, E. K., Su, X., Vereijken, B., Bach, K., and Nilsen,
J. H. (2020). Comparison of a deep learning-based
pose estimation system to marker-based and kinect
systems in exergaming for balance training. Sensors,
20(23):6940.
ICT4AWE 2022 - 8th International Conference on Information and Communication Technologies for Ageing Well and e-Health
176
