
The Role of Culture in User Adoption of Mobile Applications for
Self-management of Health: A Conceptual Framework
Mariam Jacobs-Basadien
a
and Shaun Pather
b
Department of Information Systems, University of the Western Cape, Robert Sobukwe Road, Belville, South Africa
Keywords: Unified Theory of Acceptance and Use of Technology 2 (UTAUT2), Self-Management, Culture, Technology
Adoption, Hofstede’s Cultural Dimensions.
Abstract: There are increasing calls to harness Information and Communications Technology (ICTs) more effectively
towards the attainment of the Sustainable Development Goals (SDGs) through innovative digital health
strategies. Diabetes mellitus, is one example of a global health problem that is increasing rapidly, affecting
the poor and disadvantaged populations the most. Self-care practices for diabetes self-management are
important to implement in one’s daily life as morbidity and mortality are preventable. Diabetes complications
and early fatalities are preventable through proper diabetes management and lifestyle modification. Mobile
health applications have been proposed as an important emergent technology to assist in self-care activities
of diabetes patients. However, the uptake and usage of mobile health (m-health) applications for self-
management of disease is low, especially among communities who are considered to be poor and
economically marginalised. This paper posits that individual’s culture persuasions have an influence on
diabetes patient’s decision to adopt and use mobile applications for diabetes self-management. A conceptual
framework is developed to understand the role of culture in the adoption of m-health mobile applications for
the self-management of disease.
1 INTRODUCTION
Since the advent of mobile phone, mobile-health (m-
health) has increasingly come under focus of health
care systems around the world as a means of
transforming the way health care is managed and
delivered. m-Health has therefore become prominent
in the literature emerging as a central element of
electronic health (e-health). M-health applications
can serve as a useful tool in the health care sector, as
they can help people manage their chronic conditions.
The literature provides evidence that it is a useful tool
to be used to decrease Non-Communicable Disease
(NCD) risk factors (Zhao et al., 2016). For example
Waki et al. (2014) aver that it plays an important role
in supporting the achievement of health-related goals
such as improving glycaemic levels of diabetes
patients. The American Association of Diabetes
Educators (AADE) (1997) which includes healthy
eating, being active, monitoring, taking medication,
problem solving, healthy coping, and reducing risks
is important for successful self-management.
a
https://orcid.org/ 0000-0003-4177-550X
b
https://orcid.org/ 0000-0002-4667-222X
However, for any individual to self-manage their
conditions, they have to first accept and use the
technology (Dou et al., 2017). However, there are
indications of levels of low uptake and use of
Information and Communication Technologies
(ICTs) among people with NCDs who are from poor
and under-resourced communities. While diabetes
affects all population groups, the demographic data
indicates that the elderly have more difficulty in using
mobile applications to manage their diabetes
(Petersen, et al., 2019).
There are several factors that have an influence on
the adoption of technology, including those in
relation to culture. For example, globally, people
have different traditions, values, religious practices
eating habits and social customs. Therefore, these
factors point to there being additional influences that
affect the adoption of mobile health (m-health)
applications (Abdulrehman et al., 2016; Ung, 2017).
According to Dehzad et al. (2014), cultural beliefs of
people are known to be key factors that influence
technology uptake and adoption. Essentially, the
Jacobs-Basadien, M. and Pather, S.
The Role of Culture in User Adoption of Mobile Applications for Self-management of Health: A Conceptual Framework.
DOI: 10.5220/0011039300003188
In Proceedings of the 8th International Conference on Information and Communication Technologies for Ageing Well and e-Health (ICT4AWE 2022), pages 37-49
ISBN: 978-989-758-566-1; ISSN: 2184-4984
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
37
cultural background influences a number of aspects of
people’s lives, including beliefs, behaviour, perception
and attitudes towards health (Swierad et al., 2017).
Researchers have investigated culture and the role
of cultural differences in the adoption and acceptance
of Information Technology. Research indicates that
cultural backgrounds play an imperative role in
affecting the uptake and use of technology (Al-
jumeily & Hussain, 2014; Masimba et al., 2019;
Tarhini et al., 2017). These studies illustrate that
cultural backgrounds play an imperative role in
influencing the uptake and use of technology
(Masimba et al., 2019). While there are ample studies
in the literature regarding technology adoption in
varying contexts, there is a dearth of understanding
concerning adoption in the context of Non-
Communicable Disease management. Importantly,
the notion of culture in relation to mobile technology
use, for a personal diseases management is closely
linked to factors that are of an individualised nature,
such as one’s cultural persuasions. However there is
scant evidence to date to understand the latter. While
there is ample understanding of technology adoption
constructs, and a fair understanding of the concept of
culture, there is no research that has conceptually
aligned the two concepts. This is the central problem
this paper addresses by presenting a framework to
understand the role of culture in application adoption
for self-management of health.
The paper is organized as follows: First, the
technology adoption models are discussed. Second,
culture and the cultural models are identified.
Thereafter, the technology adoption models are
compared and the cultural models; Two of the often
cited research are assessed and compared with each
other, viz. Hofstede’s cultural dimensions (1980,
2010) and Trompenaars & Hampden-Turner cultural
model (1997). Subsequently, understanding culture
within a country context is discussed. Next, the
Unified Theory of Acceptance and Use of
Technology 2 (Venkatesh et al., 2012) is mapped
against Hofstede’s cultural dimensions to identify the
relationships between them. This is the foundation on
which a conceptual model is derived.
2 USER ACCEPTANCE OF
TECHNOLOGY MODELS
Technology acceptance is defined as a user’s
intention to use and continue making use of a
particular IT product (Davis, 1989) (e.g., a mobile
phone or computer).
Technology acceptance has been an important
subject in IS research. It has been studied since the
1970s in the field of computer science where studying
the adoption, acceptance and use of Information
Systems (IS) is an area of study in the software
engineering field (Momani & Jamous, 2017). The
mainstreaming of technology and the importance of
the people dimension in terms of gaining benefit from
the use of technology rose to the fore when
researchers such as Venkatesh et al. (2003) found that
users were not deriving benefits from technology.
Historically, this area of research focuses on the
problem that the availability of technology does not
necessarily convert into adoption and use.
Understanding the reasons why users accept or reject
information technology is one of the crucial areas in
IS research (Venkatesh et al., 2007). In the study of
m-health acceptance, understanding technology
adoption and usage is essential. Venkatesh et al.
(2016) have stated that users must first use
technology before the desired outcome can be
achieved.
Technology adoption models have been
developed to understand how users understand,
accept and use technology (Venkatesh et al., 2003).
In addition, these models introduce factors that can
affect user decisions to adopt new technologies.
Models such as the technology acceptance model
(TAM) developed by (Davis, 1989) explain user
acceptance of new technologies. Even though there
have been many studies conducted using technology
adoption models, it is crucial to understand how the
models have evolved throughout the years as this
reveals the similarities and differences between them.
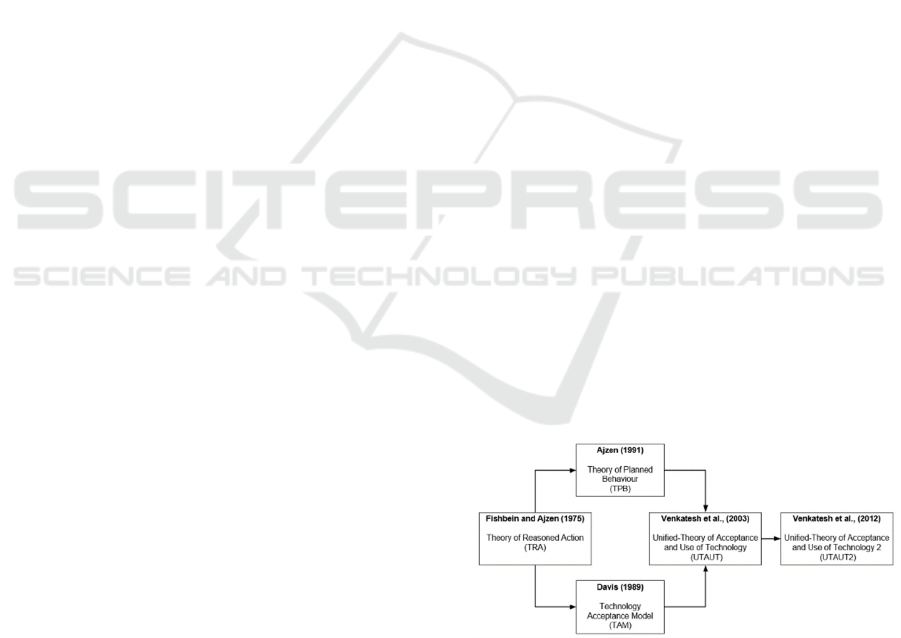
Figure 1 represents the dominant technology adoption
models in the area of m-health and how it evolved
over time.
Figure 1: The prominent technology adoption models over
time.
The above figure depicts that the Unified-Theory
of Acceptance and Use of technology (UTAUT) was
developed based on prior models such as the theory
of reasoned action (TRA), technology acceptance
model (TAM) and the theory of planned behaviour
ICT4AWE 2022 - 8th International Conference on Information and Communication Technologies for Ageing Well and e-Health
38
(TPB). The UTAUT was then extended to the
UTAUT2. The similarities between the five
prominent models are discussed in Table 1 section,
section 4.
The succeeding section discusses the Unified-
Theory of Acceptance and use of Technology 2 which
is conceptually a central aspect of this study.
2.1 Unified-Theory of Acceptance and
Use of Technology 2
Unified-Theory of Acceptance and Use of
Technology (UTAUT) was believed to be a complete
model to forecast IT acceptance (Martins et al., 2014)
until Unified-Theory of Acceptance and Use of
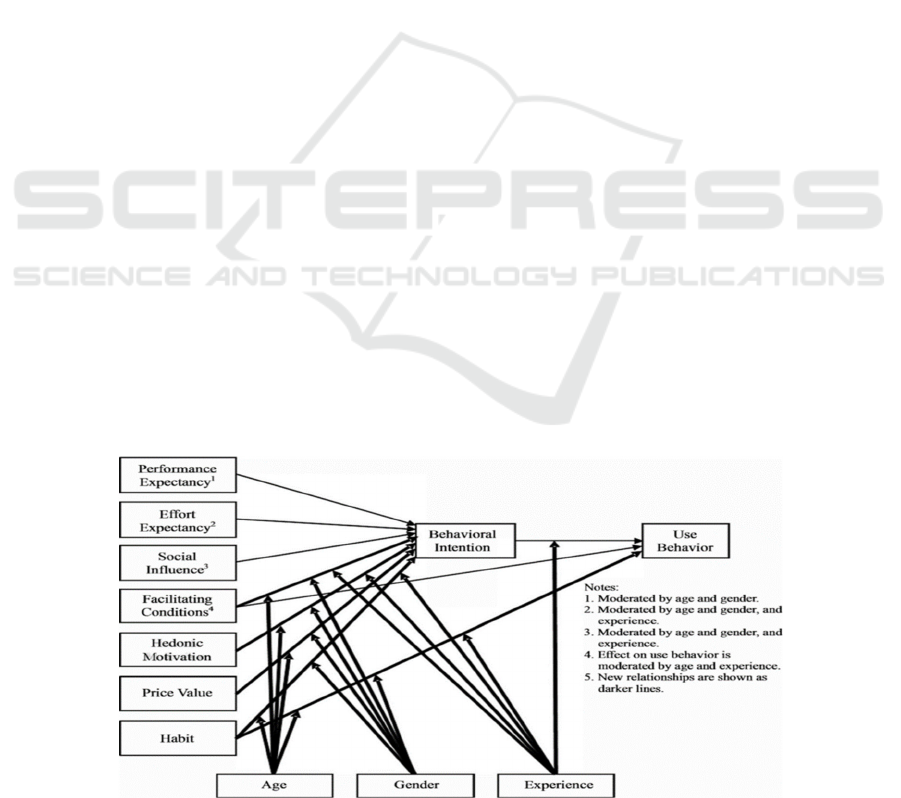
Technology 2 was developed. The Unified- Theory of
Acceptance and Use of Technology 2 model
(UTAUT2) (Figure 2) is an extension of the UTAUT
for understanding consumer acceptance of new
technology better, and is centred on the individuals’
perspectives of technology adoption (Venkatesh et
al., 2012). The UTAUT2 includes three additional
moderators: hedonic motivation, price value and
habit.
Hedonic motivation was regarded as a significant
predictor in prior research (Venkatesh et al., 2003),
and it was integrated into the Unified-Theory of
Acceptance and Use of Technology 2 (UTAUT2) for
more stressing utilities. The price value construct was
introduced in the UTAUT2 model as the quality of
the product, cost and utility compared with the price
will in turn influence adoption decisions (Hennigs et
al., 2013). Habit is a significant predictor of mobile
internet use (Venkatesh et al., 2012, 2016) and has
appeared to be the strongest determining factor of
individual technology use (Tamilmani et al., 2020).
In the UTAUT2, habit is assumed to directly
influence both behavioural intention and use
behaviour (Hwang et al., 2016).
The UTAUT2 core constructs are defined below:
Performance Expectancy (PE): “is the degree
to which an individual believes that using the
system will help him or her to attain gains in
job performance” (Venkatesh et al., 2003,
p.447).
Effort Expectancy (EE): “is the degree of ease
associated with the use of the system”
(Venkatesh et al., 2003, p.450).
Social Influence (SI): “is the degree to which
an individual perceives that important others
believe he or she should use the new system”
(Venkatesh et al., 2003, p.451).
Facilitating Conditions (FC): “is the degree to
which an individual believes that an
organisational and technical infrastructure
exists to support the use of the system”
(Venkatesh et al., 2003, p.453).
Hedonic Motivation (HM): is defined as “the
fun or pleasure derived from using a
technology” (Venkatesh et al., 2012, p.161).
Price Value (PV): is defined as “consumers’
cognitive trade-offs between the perceived
benefits of the applications and monetary costs
for using them” (Venkatesh et al., 2012,
p.161).
Habit (HT): “the extent to which people tend
to perform behaviours automatically because
of learning” (Venkatesh et al., 2012, p.161).
The UTAUT2 model has been used to explore
various research problems such as health applications
(Dwivedi et al., 2016; Yuan et al., 2015; Pancar &
Ozkan Yildirim, 2021) and technology adoption and
culture (Baptista & Oliveira, 2015; Lai et al., 2016;
Tarhini et al., 2017; Teo & Huang, 2018).
Figure 2: The Unified-Theory of Acceptance and Use of Technology 2 (Source: Venkatesh et al., 2012, p.160).
The Role of Culture in User Adoption of Mobile Applications for Self-management of Health: A Conceptual Framework
39
3 MODELS OF CULTURE
Having set a foundational understanding of
technology acceptance in the previous section, the
next consideration is to understand culture. Amongst
other essential points identified in the literature, the
notion of culture was identified as being one of the
main conceptual gaps in one of the most often applied
models, viz. the Unified-Theory of Acceptance and
Use of Technology model (UTAUT).
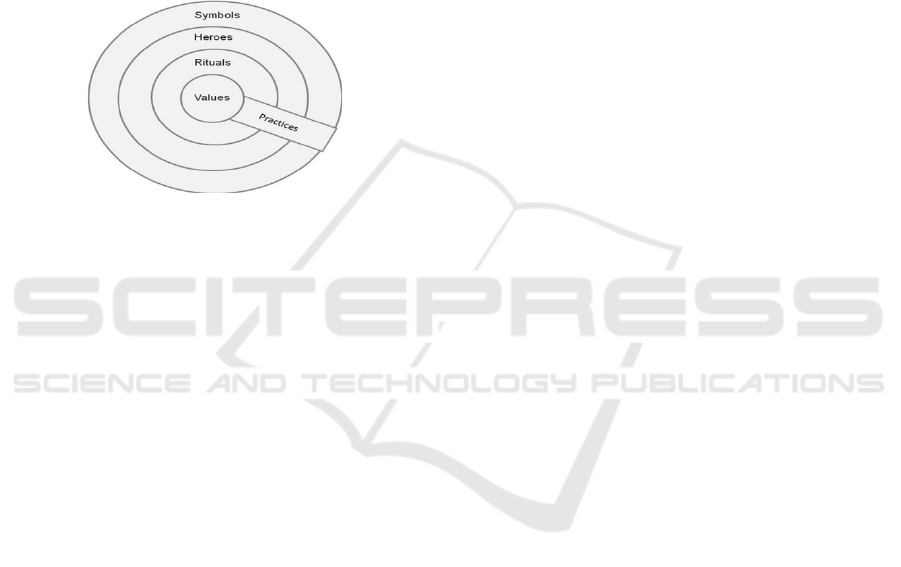
According to Hofstede et al. (2010), cultural
differences are displayed on different levels of depth
such as symbols, heroes, rituals and values (Figure 3).
Figure 3: The “Onion”: Manifestations of Culture at
Different Levels of Depth (Source: Hofstede et al. (2010,
p.8)).
The levels of depth are defined below by Hofstede et
al. (2010, p.8-9) :
Symbols: In the first, outermost layer, are pictures,
words and jargons that contain a specific meaning
that is understood by those people who form part of
the same culture.
Heroes: The second layer is defined as people
dead or alive that possesses qualities that are glorified
by people in a particular society, for example, Nelson
Mandela, the first president post- apartheid.
Rituals: The third layer is collective activities that
are seen as socially essential. The ways of greeting,
social and religious ceremonies are examples of
rituals.
Values: The fourth, innermost layer, are wide-
ranging terms that prefer certain states as opposed to
others, for example, good rather than evil.
Hofstede et al., (2010) argue that culture is
learned and not inherent. By the term “learned” they
indicate that people’s culture is adopted by the effect
of social values and personal incidents that are unique
to an individual (Hofstede et al., 2010). However, it
is argued that even though individual members
perceive culture based on what they see or hear,
culture can also be transmitted consciously or
unconsciously from one generation to another.
Beukman (2005) states that culture is two
dimensional. It can either be explicit or implicit.
Explicit consists of behavioural patterns in a given
situation and implicit is a manifestation of attitudes,
values, beliefs, and norms, which collectively give
meaning to explicit behaviour.
Hofstede posits that culture is made up of six
different layers. It can exist at a “national level or
country level, a regional and/or ethnic and/or
religious level, a gender level, a social class level, an
organisational level, and lastly an individual level”
(Hofstede et al., 2010, p.18). At a country level,
culture functions through religions, languages, and
social structures (Hassan et al., 2016). Some markers
distinguish one individual from another in a given
society such as their demographics, educational
background, religion, location and income status
(Hodgetts et al., 2005).
As culture exists differently in all parts of the
world, American, Asian, European and African
culture is unique in all forms and expressions (Yavwa
& Twinomurinzi, 2018). Culture, as a social concept,
has been studied for many years. Research findings
have found that there is a link between culture and
technology adoption. Culture can either impede
technology adoption (Hasan & Ditsa, 1999) or can
facilitate technology acceptance (Sriwindono &
Yahya, 2012). It is, therefore, vital to incorporate
culture into the models of user acceptance.
3.1 Hofstede’s Cultural Dimensions
Hofstede’s definition of culture is broad and has been
widely accepted in IS literature. He defines culture as
“the collective programming of the mind which
distinguishes the members of one human group from
another” (Hofstede, 1980, p.13). Hofstede (1980)
developed an index model and presented four cultural
values of culture: Power Distance, Individualism
versus Collectivism, Masculinity versus Femininity,
and Uncertainty Avoidance. Hofstede then included
Long-Term versus Short-Term Orientation as a fifth
dimension (Hofstede, 2001). He later added
Indulgence versus Restraint as a sixth dimension
(Hofstede et al., 2010).
Hofstede et al. (2010) have defined cultural values
as follows:
Power Distance:
“extent to which the less
powerful members of institutions and organisations
within a country expect and accept that power is
distributed unequally” (p.61).
Individualism- collectivism: “refers to societies in
which the ties between individuals are loose:
everyone is expected to look after him or herself and
his or her immediate family. Collectivism as its
opposite pertains to societies in which people from
ICT4AWE 2022 - 8th International Conference on Information and Communication Technologies for Ageing Well and e-Health
40

birth onward are integrated into strong, cohesive in-
groups, which throughout people’s lifetime continue
to protect them in exchange for unquestioning
loyalty” (p.92).
Masculinity- femininity: Masculinity refers to a
“society in which emotional gender roles are clearly
distinct” (p.519). Femininity is seen as a “society in
which emotional gender roles overlap: both men and
women are supposed to be modest, tender, and
concerned with the quality of life” (p.517).
Uncertainty avoidance: “the extent to which the
members of a culture feel threatened by ambiguous or
unknown situations” (p.191).
Long-term orientation- Short-term orientation:
“the fostering of virtues oriented toward future
rewards—in particular, perseverance and thrift”
(p.239). Short-term orientation “the fostering of
virtues related to the past and present—in particular,
respect for tradition, preservation of face, and
fulfilling social obligations” (p.239).
Indulgence- restraint: Indulgence refers to a
“society that allows relatively free gratification of
basic and natural human desires related to enjoying
life and having fun” (p.519). Restraint refers to a
“society that suppresses gratification of needs and
regulates it by means of strict social norms” (p.521).
Hofstede’s culture framework has been
extensively studied in the areas of Information
Systems (IS) and Information Technology (IT)
studies (e.g. (Lee et al., 2013; Sriwindono & Yahya,
2012, 2014; Tarhini et al., 2017)). These studies
suggest that a significant relationship exists amongst
national culture and the rate of technology adoption
and acceptance.
In a study carried out by Sriwindono & Yahya,
(2012), long-term orientation has been found to have
the highest effect on perceived usefulness of
technology, then followed by power distance and
individualism on perceived ease of use of technology.
Although Hofstede’s cultural values have been
influential in many disciplines, they have not escaped
criticism. Hofstede work has been criticised for a lack
of generalisability and over- simplifying culture (Ng
et al., 2007). Furthermore, Hofstede (1980) stated that
a country-level analysis is unable to predict individual
behaviour. However, national cultural values have
been examined as being espoused at the individual
level in previous research (Srite & Karahanna, 2006;
Sun et al., 2019; Teo & Huang, 2018). Later,
Hofstede recommended that culture should be
investigated at the social level and values should be
studied at the individual level (Hofstede, 2001). He
further claimed that cultural values are the foundation
of daily practices (Figure 3 - the onion model), and
daily practice was affected by a person’s cultural
values (Hofstede, 2001).
The application of Hofstede’s cultural dimensions
to diabetes patients self-care behaviour activities are
discussed in the appendix.
3.2 Trompenaars & Hampden-Turner
Cultural Dimensions
Trompenaars & Hampden-Turner (1997) cultural
model was developed to explain cultural differences
based on the challenges people encounter when
forming social communities. According to
Trompenaars & Hampden-Turner, “culture is the way
in which a group of people solve problems and
reconcile dilemmas” (Trompenaars & Hampden-
Turner, 1997, p.6). They further state that preferences
differentiate people into various cultural dimensions.
These dimensions were then developed to illustrate
the differences between one culture compared to
another and how culture relates to societal level
characteristics. The dimensions illustrated by this
model are useful in comprehending how people from
different national cultures interact.
The Trompenaars & Hampden-Turner (1997)
model consist of seven dimensions:
Individualism versus Communitarianism: In
Individualism describes cultures where ties between
individuals are loose. The individual rather than any
group norms determine decision making on lifestyle.
In Communitarian cultures, groups are considered to
be the most important, unlike individuals. As
Communitarian refers to groups, rewards are given to
group performance, decisions are taken collectively,
and individual performances are not publicly praised
(p.9).
Universalism versus Particularism: In a
Universalistic culture, people abide by standards that
are collectively decided upon by all who form part of
this culture. This culture consists of laws, values and
rules and which are applied to everyone.
Alternatively, in Particularistic cultures, personal
relationships are valued as a substitute for laws and
rules (p.8).
Specific versus Diffuse: In specific culture, people
believe that their private lives ought to be kept
separate from their professional lives. In diffuse
oriented culture, personal and professional
relationships overlap (p.9).
Affectivity versus Neutrality: In Affectivity
cultures, people are allowed to display their emotions
to others and may partially allow emotions to
influence their decision. While in neutral cultures,
The Role of Culture in User Adoption of Mobile Applications for Self-management of Health: A Conceptual Framework
41
individuals should practice self-control regarding
their emotions (p.69).
Internal direction versus External direction: In
internal-directed cultures, to achieve goals people
deem that they can control their surroundings while
in external direction, people deem that they are
controlled by their surroundings.
Achieved Status versus Ascribed Status: In
achievement cultures, status is given based on how
well people perform at a particular task. While in
Ascription culture, people are endorsed on what or
who they are. Status may be conferred according to
demographics, family and racial group (p.102).
Sequential Time versus Synchronic Time: In a
sequential time culture, people tend to be inflexible.
The sequence of events is of utmost importance in this
regard, as individuals value planning and punctuality
as imperative. In contrast, people who view plans and
obligations as flexible form part of a Synchronic time
as they work on multiple tasks at once (p.124).
An assessment of the above indicates that, in
relation to the study, Trompenaars & Hampden-
Turner (1997) cultural dimensions may be a relevant
model to study culture in this context. The application
of Trompenaars and Hampden-Turner cultural model
to diabetes patients’ self-care activities are discussed
in the appendix.
The similarities between Trompenaars &
Hampden-Turner cultural model and Hofstede’s
cultural dimensions are discussed in the next section
(section 4, Table 2).
4 COMPARISON OF USER
ACCEPTANCE MODELS AND
CULTURAL MODELS
Table 1 presents the five prominent models. This
includes the key constructs of the user acceptance
model who were found to have some alignment to the
study research problem.
Through the comparison of the user acceptance
models, the TRA is similar to that of the TPB. The
TPB can be compared to the UTAUT model as the
key constructs (PE, EE and Social Influence) of the
UTAUT model is similar to that of the TPB model.
An examination of the definitions of the constructs
indicates that “attitude” represents “performance
expectancy” and “effort expectancy” constructs in the
UTAUT model because PE and EE are attitudinal
constructs. “Subjective norm” in the TAM is similar
to the Social Influence (SI) construct in the UTAUT
model, and the “perceived behavioural control”
Table 1: Comparison of the user acceptance model.
TRA
TPB
TAM
UTAUT
UTAUT 2
Key constructs
Attitude
towards
behaviour (A)
✔
✔
PU
P
E and
EE
PE and
EE
Subjective
norms (SN)
✔
✔
SI
S
I
Perceived
behavioural
control (PBC)
✔
PEOU EE EE
Perceived ease
of use (PEOU)
PBC
✔
EE EE
Perceived
usefulness
(PU)
A
✔
PE PE
Performance
expectancy
(PE)
✔
✔
Effort
expectancy
(EE)
✔
✔
Social
influence (SI)
✔
✔
Facilitating
conditions
(FC)
✔
✔
✔
Hedonic
Motivation
(HM)
✔
Price value
(PV)
✔
Habit (H)
✔
construct is similar to that of facilitating conditions in
the UTAUT model (Sun et al., 2013). Furthermore,
both the TPB and UTAUT models have been used in
the area of health research and Information
Technology adoption.
Table 2 presents the similarities between
Hofstede’s cultural dimensions and Trompenaars &
Hampden-Turner’s cultural model.
ICT4AWE 2022 - 8th International Conference on Information and Communication Technologies for Ageing Well and e-Health
42
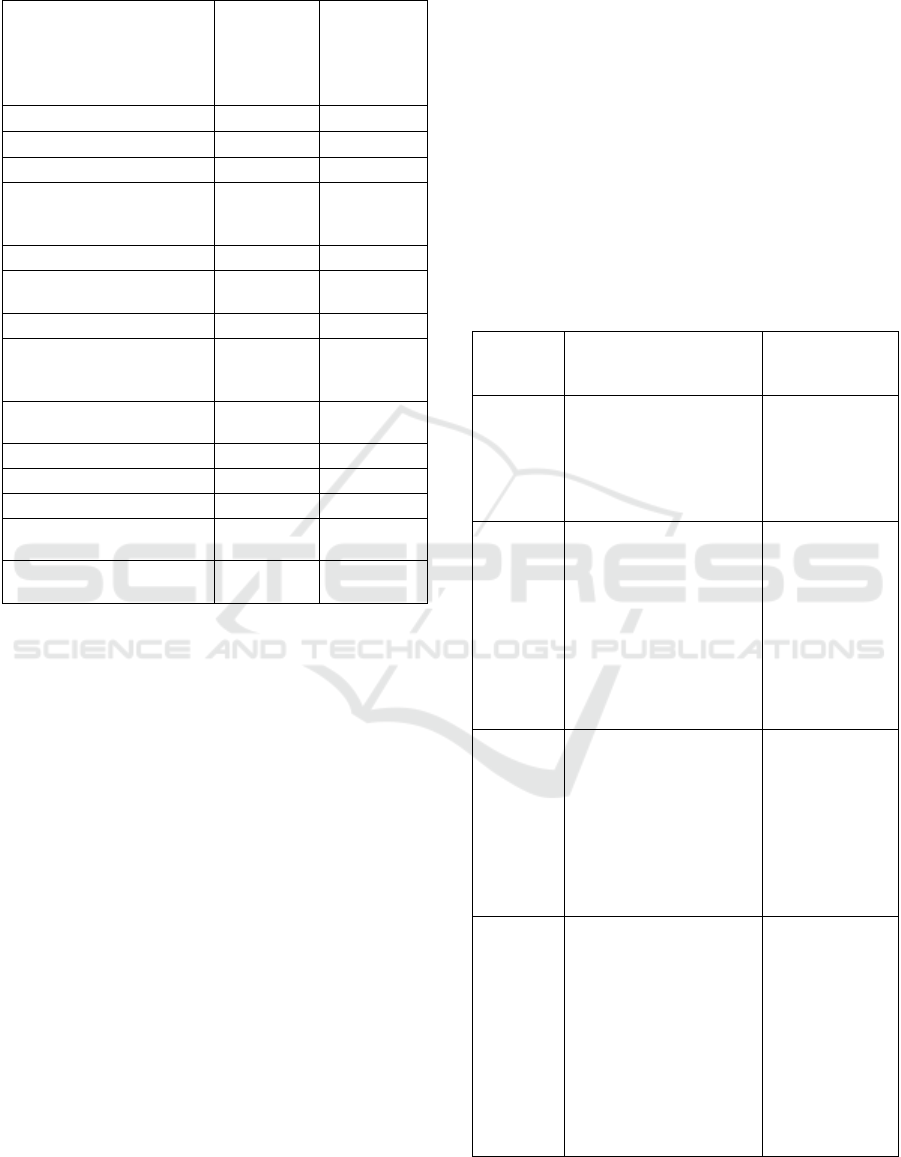
Table 2: Comparison of Hofstede's cultural dimensions and
Trompenaars & Hampden-Turner cultural model.
Hofstede
cultural
dimensions
Trompenaars
& Hampden-
Turner
Cultural
model
Dimensions of culture
Power
Distance
✔
Individualism -collectivism
✔ ✔
Masculinity -Femininity
✔
Similar to
affectivity/
neutralit
y
Uncertainty
avoidance
✔
Long term orientation -
Short term orientation
✔
Indulgence -Restraint
✔
Individualism vs
communitarianism
Similar to
Individualism
-collectivis
m
✔
Universalism versus
Particularism
✔
Specific versus Diffuse
✔
Affectivity versus Neutrality
✔
N
ature Orientation
✔
Achieved Status versus
Ascribed Status
✔
Sequential Time versus
S
y
nchronic Time
✔
In regard to the cultural dimensions, Trompenaars &
Hampden-Turner, individualism versus
communitarianism and universalism versus
particularism dimensions are similar to Hofstede’s
cultural individualism– collectivism dimensions. In
addition, affectivity versus neutrality is similar to
Hofstede’s cultural masculinity–femininity. As
previously mentioned, Hofstede’s constructs have
been used to study the relationship between culture
and technology adoption. Based on the cultural
dimension of individualism versus collectivism,
culture may likely have some influence on attitude
toward technology use (Bandyopadhyay &
Fraccastoro, 2007).
Both men and women can exhibit masculine and
feminine traits (Cyr et al., 2017) and this can
influence technology adoption. Furthermore,
Hofstede’s construct, uncertainty avoidance has
received much attention in the field of technology
adoption (Özbilen, 2017). It has been found that
informational influence from family can encourage
people in uncertainty avoidance cultures to adopt and
use technologies (Alhirz & Sajeev, 2015). On the
other hand, Trompenaars & Hampden-Turner (1997)
has received little attention. Furthermore, this
framework does not provide an applied approach to
measure culture (Su & Sauers, 2009).
5 INTEGRATING CULTURE AT
AN INDIVIDUAL LEVEL WITH
THE MODELS FOR USER
ACCEPTANCE
Table 3 represents the user acceptance models that
have been used together with cultural models to
answer various research questions
Table 3: Studies on culture and technology in different
contexts.
Author
Constructs used in this
study
Methodology
and models
used
Sun et al.
(2019)
Individual-level Culture
Hofstede cultural
dimensions Perceived
usefulness
Perceived ease of use
Technology
Acceptance
Model Hofstede
Questionnaire
Zhang et
al. (2018)
Performance expectancy
Effort expectancy
Social influence
Perceived risk Trust
Hofstede’s cultural
dimensions
Unified- Theory
of Acceptance
and Use of
Technology
Hofstede’s
cultural
dimensions
Questionnaire
Teo &
Huang
(2018)
Hofstede cultural
dimensions Perceived
ease of use Perceived
Usefulness
Attitude towards use
Behavioural intention
Extended
Technology
Acceptance
Model
Hofstede
cultural Model
Questionnaire
Lu et al.
(2017)
Age, gender, experience
Hofstede’s cultural
dimensions Perceived
effort expectancy
Perceived performance
expectancy
Perceived mobile social
influence Perceived
privacy protection
Espoused
cultural
dimension of
Hofstede
Unified- Theory
of Acceptance
and Use of
Technology
Questionnaire
The Role of Culture in User Adoption of Mobile Applications for Self-management of Health: A Conceptual Framework
43
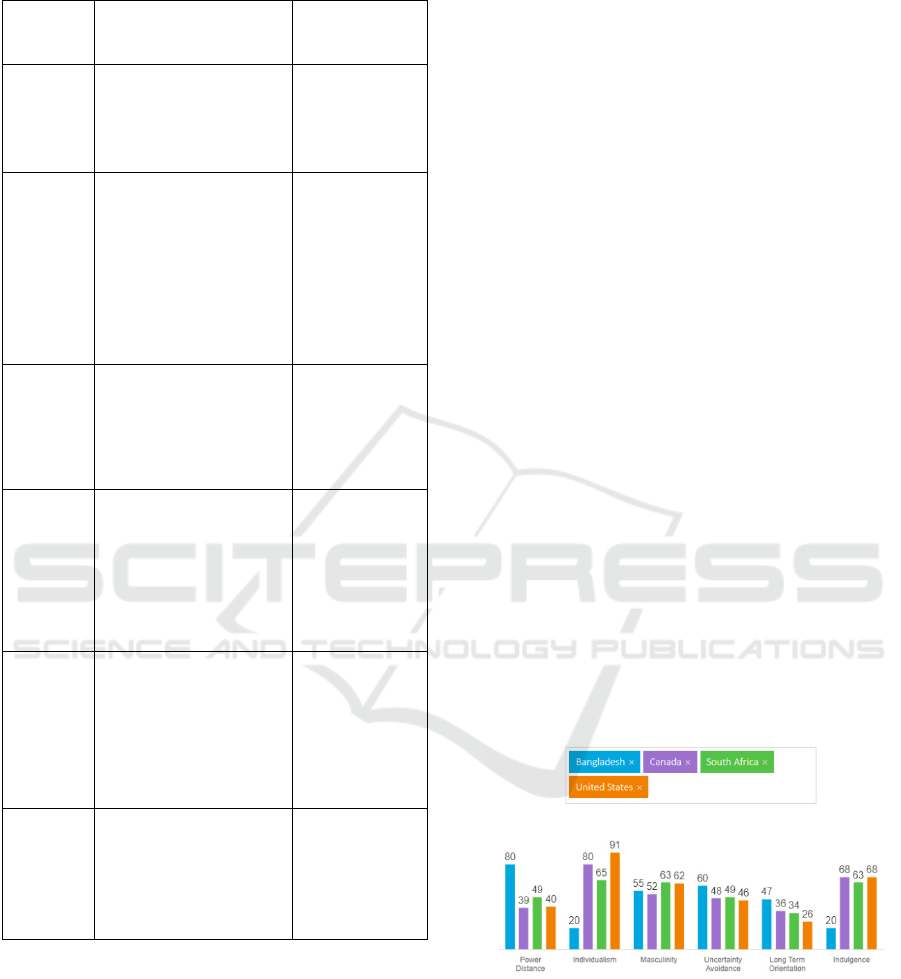
Table 3: Studies on culture and technology in different
contexts (cont.).
Author
Constructs used in this
study
Methodology
and models
used
Tarhini et
al. (2017)
Individual-level culture
Perceived ease of use
Subjective norms
quality of work-life
Behavioural Intention
Technology
Acceptance
Model
Questionnaire
Lai et al.,
(2016)
Long-term orientation
Collectivism
Power Distance
Uncertainty avoidance
Performance expectancy
Effort expectancy
Social influence Hedonic
Motivation
Facilitating conditions
Hofstede
cultural
dimensions
UTAUT2
Survey
Baptista &
Oliveira,
(2015)
UTAUT2
Hofstede cultural
dimensions Behavioural
intention
Use behaviour
UTAUT2
Hofstede
cultural
dimensions
Questionnaire
Hoehle et
al. (2015)
Uncertainty avoidance,
Perceived usefulness
Perceived ease of use
Perceived usefulness
Collected data
from consumers
using ICT in
four countries,
Hofstede
cultural
dimensions
Al-jumeily
&
Hussain,
(2014)
Individualism-
Collectivism, Uncertainty
Avoidance
Power Distance
Perceived usefulness
Perceived ease of use
Technology
Acceptance
Model Hofstede
cultural
dimensions
Survey
Al-
Gahtani et
al., (2007)
Hofstede cultural
dimensions Unified-
Theory of Acceptance
and Use of Technology
Unified-Theory
of Acceptance
and Use of
Technology
Survey
By an assessment, it can be noted that Hofstede’s
cultural dimension can be used in studies of culture
and technology adoption (Table 3). The methodology
that many of the studies adopted has been a
questionnaire method approach. Previous studies
have used the Technology Acceptance Model (TAM)
and the Unified-Theory of Acceptance and Use of
Technology (UTAUT) as a lens for analysis.
However, it has been found that the TAM model is
unable to forecast technology use across every culture
(Straub et al., 1997). To understand diabetes self-
management in marginalised communities,
challenges such as cultural backgrounds and beliefs
should also be considered.
Hofstede’s cultural model has been used in studies
relating to technology adoption in various contexts as
Hofstede’s cultural dimensions aid researchers to
comprehend what motivates technology adoption and
use (Hoehle et al., 2015; Leidner & Kayworth, 2006).
Additionally, Hofstede’s constructs allow scholars to
study issues in a variety of phenomena (Hoehle et al.,
2015). Literature indicates that many studies focusing
on culture and technology adoption have used
Hofstede’s cultural dimensions (e.g. Srite &
Karahanna, 2006; Sun et al., 2019; Tarhini et al.,
2017). A recent study by Alam et al. (2020) explored
factors affecting the adoption of m-health in a
developed country. The authors recommend that
further research ought to be done in different socio-
economic groups, rural areas and other cultures and
groups with different religious beliefs. Petersen et al.,
(2019) suggested that further research should be
conducted on culture in the use of m‐health for
diabetes self‐ management.
6 UNDERSTANDING CULTURE
WITHIN COUNTRY
CONTEXTS
Culture manifests differently across nations. Figure 4
depicts that culture in developing countries (South
Africa and Bangladesh) differs from developing
countries (Canada and United States).
Figure 4: Hofstede's insights (Source: Hofstede, 2019).
There is a low power distance value for South
Africa, Canada, and the United States. The value
indicates that people accept hierarchical order
(Hofstede, 2019). Context-wise, diabetic patients
from low power distance countries are likely to
conform to the opinions and decisions of their health
care professional.
ICT4AWE 2022 - 8th International Conference on Information and Communication Technologies for Ageing Well and e-Health
44

The individualism dimension indicates that
people care for themselves and immediate family
(Hofstede, 2019). In Bangladesh, the value shows that
people conform more towards a collectivism culture.
This suggests that diabetic patients will conform to
the decisions of their society, or communities in
which they live. In the remaining countries, the data
suggests that the decisions are made at the
individual’s discretion.
The masculinity dimension indicates that people
“live to work” (Hofstede, 2019). All four countries
score high in this dimension which indicates that
individuals will prioritise work over other matters.
This for example, could imply that a diabetic patient
in such a country may not prioritise the use of tools
such as m-health applications for disease self-
management.
The uncertainty avoidance dimension indicates a
high value for Bangladesh and suggests that people in
this country fear uncertainty. A consequence of such
a cultural persuasion implies that people may shun
new technologies and innovations if the adoption and
uptake thereof is associated with uncertainty.
South Africa and the United States indicates low
long-term orientation which indicates that traditions
are more important, and change is viewed adversely.
Therefore, if one considers this cultural dimension in
the case of diabetic patients, it could imply that they
would prefer traditional face-to-face consultations
with doctors as compared to using technology to
manage their health condition.
South Africa, United States and Canada illustrates
a culture of indulgence which indicates that people in
these countries prefer having a good time and
spending their time as they wish. In the context of
this study’s problem this could imply that if persons
engage in self-care behaviour, including using
technology for it, they will ensure that they make
decisions that provide them with fulfilment and
satisfaction.
7 MAPPING UNIFIED-THEORY
OF ACCEPTANCE AND USE OF
TECHNOLOGY 2 AGAINST
HOFSTEDE’S CULTURAL
DIMENSIONS
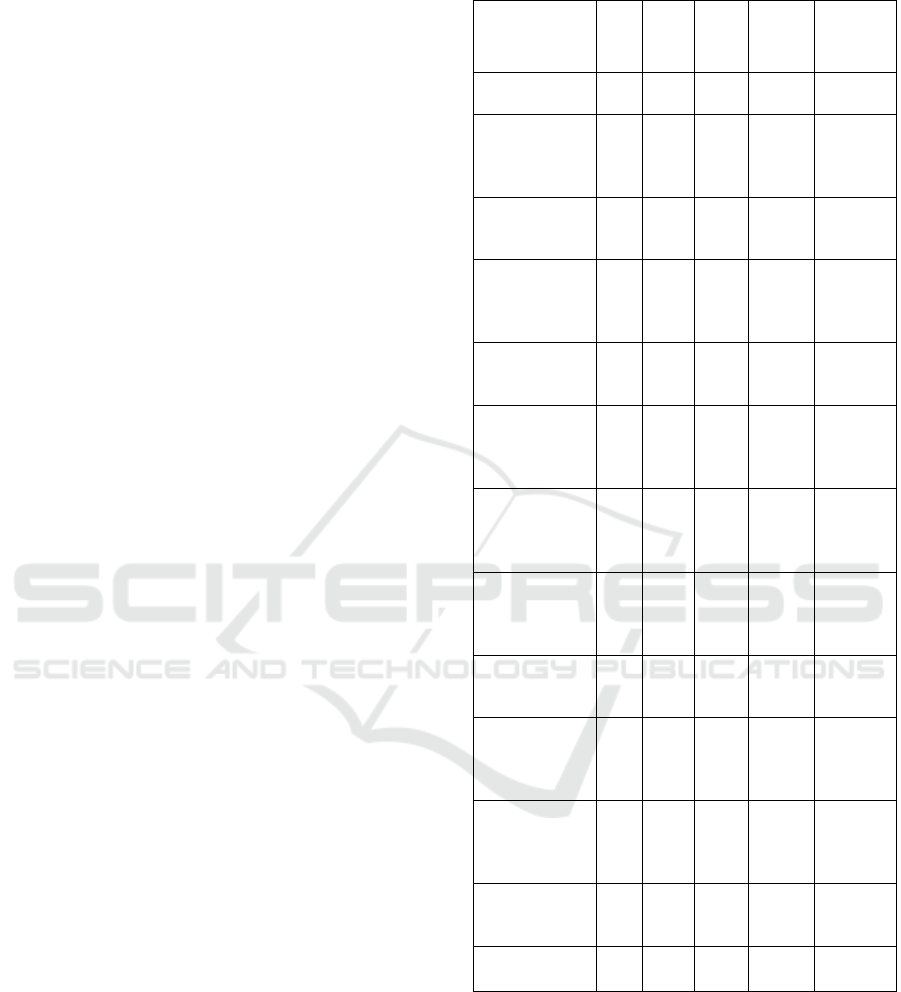
Table 4 presents the outcome of this. It maps the
seven constructs of the Unified-Theory of
Acceptance and Use of Technology 2 (UTAUT2)
against Hofstede’s cultural dimensions in order to
assess which of the theoretical definitions of the
Hofstede’s cultural dimensions fit against the
UTAUT2 technology adoption (as depicted by
UTAUT2) amongst diabetic patients in previously
disadvantaged communities.
Table 4: Mapping UTAUT2 constructs against Hofstede’s
cultural dimensions.
Utaut2
Hofstede
PE EE SI
FC
HM PV H
Power Distance
X
Individualism-
Collectivism
X
X
Masculinity
Femininity
X
Uncertainty
avoidance
X
X
Long term
orientation -
Short term
orientation
X
Indulgence
- Restraint
X
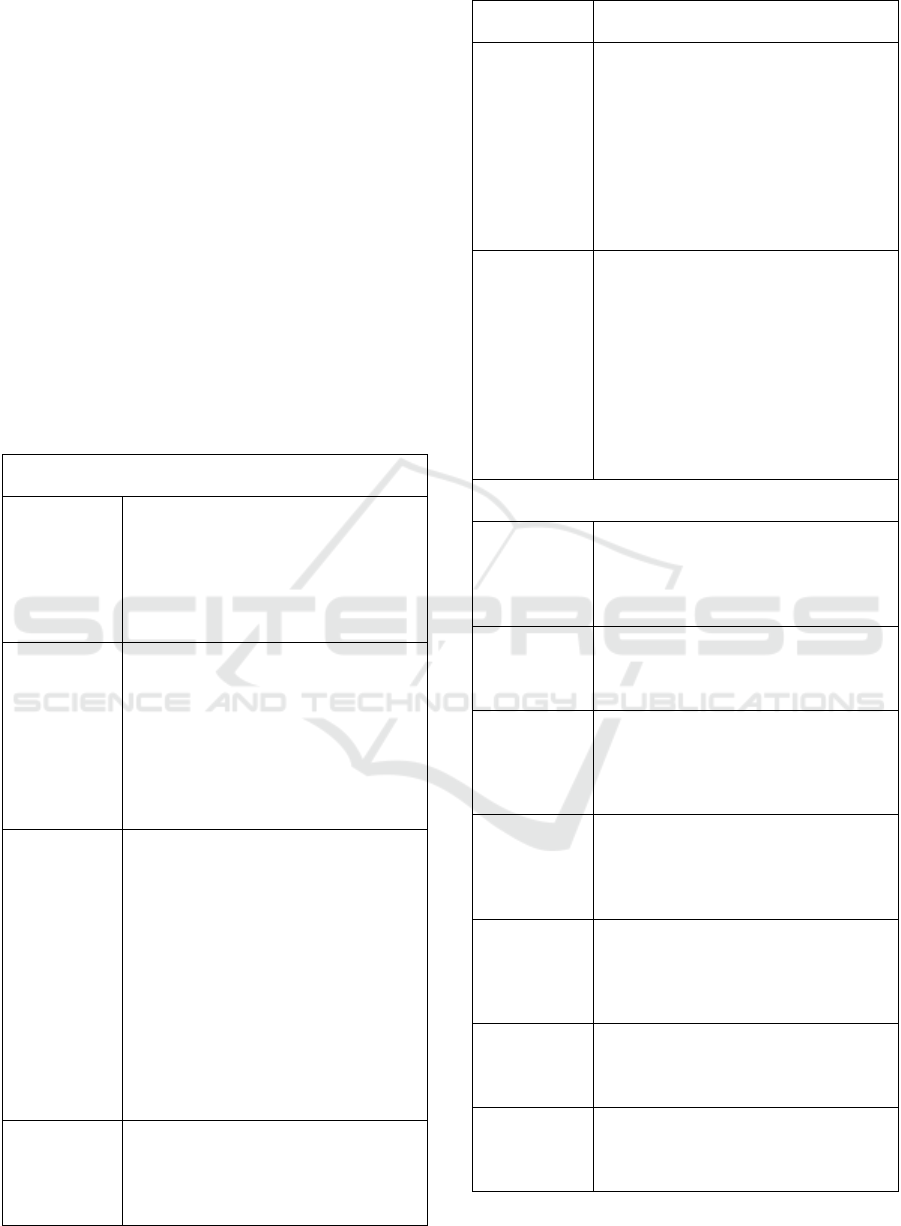
8 CONCEPTUAL FRAMEWORK
The underpinning theoretical framework from the
extant literature (Figure 2) and Hofstede’s cultural
dimensions (Section 3.1) provide a basis for the
conceptual framework below. Figure 5 is conceived
from the foregoing analyses (Sections 4, 5 and 7). It
provides a conceptual foundational understanding of
how the dimensions of culture influence technology
adoption in the context of self-management of NCDs
such as diabetes.
The literature review presented evidence that the
UTAUT2 is the best suited model to study technology
adoption and culture. After reviewing literature on
culture, Hofstede’s cultural dimensions have been
deemed as an appropriate fit to study culture in the
context of technology acceptance.
Looking ahead, researchers should consider
empirical investigations into the problem area as
follows:
There are six concepts that explain the
phenomenon of culture. In investigating such
problems in the field all of these must be taken
into account to understand whether and how
diabetes patients’ culture influences their self-
care behaviours and whether their culture
influences their m-health acceptance and usage
for their self-management.
The Role of Culture in User Adoption of Mobile Applications for Self-management of Health: A Conceptual Framework
45
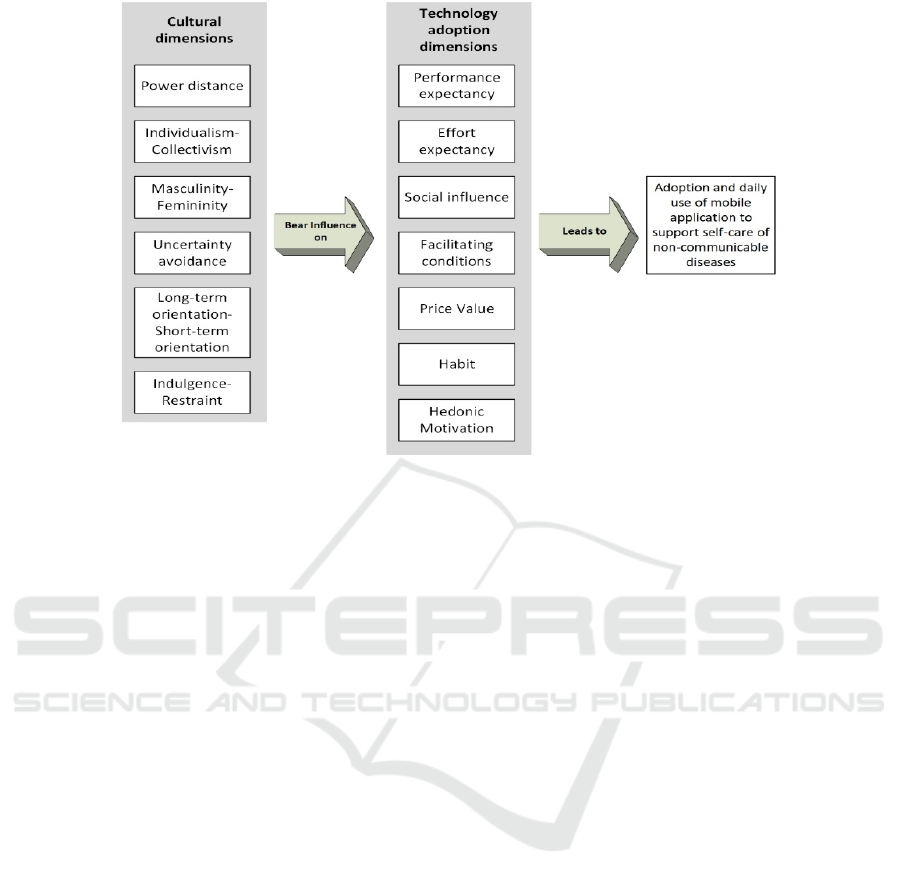
Figure 5: A conceptual framework of the role of culture on mobile technology acceptance and use.
Seven constructs drawn from the Unified-
Theory of Acceptance and Use of Technology 2
provide insight into diabetes patients acceptance
and usage of m-health to self- manage their
condition.
Finally, the AADE 7 self-behaviour activities
provide a framework of actual day to day living
of people with NCDs. These provide the
context in which to study the concepts of culture
and technology acceptance.
9 CONCLUSIONS
This paper derived a conceptual framework to explain
the problem of how culture influences technology
adoption in the context of self-care behaviour
activities. The conceptual framework can serve as a
starting point to assist policymakers and application
developers to tailor mobile applications for this target
population. In addition, this model can inform and
improve current m-health related interventions,
which could result in the improved or successful
adoption and uptake of ICT, specifically m-health
applications among diabetic patients in poor and
under-resourced communities.
The paper presents a first step to address a gap in
the literature with respect to the understanding of
culture in m-health acceptance and use for health self-
management in general, and for diabetes self-
management in particular. We conclude that to
achieve effective self-management of diabetes using
a mobile application, cultural factors that prevail on
users must be taken into consideration. Therefore this
paper contributes to a better understanding of the
nexus between culture and technology adoption. The
paper furthermore contributes towards a better
understanding of how to successfully apply ICT
towards the attainment of the UN’s Sustainable
Development Goal 3.
The next step in the research process is to use the
conceptual framework and related understandings to
inform both a mobile application design process and,
importantly, how to mitigate low adoption of an
application. By understanding the role of culture in
uptake and use of m-health applications, government,
and any other stakeholders, can be informed as to how
to mitigate low adoption scenarios, by considering the
outcomes of this study. For example, effort
expectancy points to user-centred design;
performance expectancy points to application
functionality. Many of the other dimensions point to
how potential users would uptake technology e.g.
power distance points to whether and how influential
people influence users to adopt mobile applications
and uncertainty avoidance points to whether
ambiguous situations hinder people from utilising a
mobile application.
The research framework provides us with insight
not only into potential mobile application
functionality – e.g., tracking health information. The
research model will be tested in under-resourced
communities in the Western Cape, South Africa using
a co-design approach such as that proposed by
ICT4AWE 2022 - 8th International Conference on Information and Communication Technologies for Ageing Well and e-Health
46

Kyakulumbye & Pather (2022). Such marginalised
communities appear to be bearing the brunt of social
and health ills. The effective deployment of ICT
based solutions will go a long way towards
sustainable solutions to improve living conditions for
such communities.
In conclusion, the conceptual framework of this
paper can be used in the next stage of research to
undertake a further study of a mobile application
functionality requirement as needed by the aged.
That would be a first step towards creating a usable
application to be deployed in a context that accounts
for the cultural dimensions influences identified in
this paper.
REFERENCES
Abdulrehman, M. S., Woith, W., Jenkins, S., Kossman, S.,
& Hunter, G. L. (2016). Exploring Cultural Influences
of Self-Management of Diabetes in Coastal Kenya.
Global Qualitative Nursing Research, 3, 1–13.
Al-Gahtani, S. S., Hubona, G. S., & Wang, J. (2007).
Information technology (IT) in Saudi Arabia: Culture
and the acceptance and use of IT. Information and
Management, 44(8), 681–691.
Al-jumeily, D., & Hussain, A. J. (2014). The impact of
cultural factors on technology acceptance : A
technology acceptance model across Eastern and
Western cultures. International Journal of Enhanced
Research in Educational Development (IJERED), 2(4),
37–62.
Alam, M. Z., Hoque, M. R., Hu, W., & Barua, Z. (2020).
Factors influencing the adoption of mHealth services in
a developing country: A patient-centric study.
International Journal of Information Management, 50,
128–143.
Alhirz, H., & Sajeev, A. S. M. (2015). Do cultural
dimensions differentiate ERP acceptance? A study in
the context of Saudi Arabia. Information Technology
and People, 28(1), 163–194.
American Association of Diabetes Educators. (1997). Self
Care Behaviors. In Diabetes Self-Management (pp. 1–
11).
Bandyopadhyay, K., & Fraccastoro, K. A. (2007). The
Effect of Culture on User Acceptance of Information
Technology. Communications of the Association for
Information Systems, 19(23), 522–543.
Baptista, G., & Oliveira, T. (2015). Understanding mobile
banking: The unified theory of acceptance and use of
technology combined with cultural moderators.
Computers in Human Behavior, 50, 418–430.
Beukman, T. L. (2005). Chapter 3 Culture, Values and
Work-related values- a theoretical overview.
Cyr, D., Gefen, D., & Walczuch, R. (2017). Exploring the
relative impact of biological sex and masculinity–
femininity values on information technology use.
Behaviour & Information Technology, 36(2), 178–193.
Davis, F. D. (1989). Perceived Usefulness , Perceived Ease
of Use , and User Acceptance of lnformation
Technology. MIS Quarterly, 13(3), 319–340.
Dehzad, F., Hilhorst, C., de Bie, C., & Claassen, E. (2014).
Adopting Health Apps, What’s Hindering Doctors and
Patients? Health, 06(16), 2204–2217.
Dou, K., Yu, P., Deng, N., Liu, F., Guan, Y., Li, Z., Ji, Y.,
Du, N., Lu, X., & Duan, H. (2017). Patients’
Acceptance of Smartphone Health Technology for
Chronic Disease Management: A Theoretical Model
and Empirical Test. JMIR MHealth and UHealth
,
5(12).
Dwivedi, Y. K., Shareef, M. A., Simintiras, A. C., Lal, B.,
& Weerakkody, V. (2016). A generalised adoption
model for services: A cross-country comparison of
mobile health (m-health). Government Information
Quarterly, 33(1), 174–187.
Hasan, H., & Ditsa, G. (1999). The impact of culture on the
adoption of IT: An interpretive study. Journal of Global
Information Management, 7(1), 5–15.
Hassan, L. M., Shiu, E., & Parry, S. (2016). Addressing the
cross-country applicability of the theory of planned
behaviour (TPB): A structured review of multi-country
TPB studies. Journal of Consumer Behaviour, 15(1),
72–86.
Hennigs, N., Wiedmann, K. P., & Klarmann, C. (2013).
Consumer value perception of luxury goods: A cross-
cultural and cross-industry comparison. In Luxury
Marketing: A Challenge for Theory and Practice (pp.
78–99). Gabler Verlag.
Hodgetts, R. M., Luthans, F., & Doh, J. (2005).
International Management: Culture, Strategy and
Behavior W/ OLC Card MP (6
th
edition). McGraw-Hill
Companies.
Hoehle, H., Zhang, X., & Venkatesh, V. (2015). An
espoused cultural perspective to understand continued
intention to use mobile applications: A four-country
study of mobile social media application usability.
European Journal of Information Systems, 24(3), 337–
359.
Hofstede. (2019). Country Comparision- Hofstede’s
Insights.
Hofstede, G. (1980). Culture’s Consequences:
International Differences in Work-related Attitudes.
Sage.
Hofstede, G. (2001). Culture’s Consequences: Comparing
Values, Behaviors, Institutions, and Organizations
Across Nations, (2
nd
edition). Sage.
Hofstede, G., Hofstede, G. J., & Minkov, M. (2010).
Cultures and Organizations: Software of the mind (3
rd
edition). Mac-Graw Hill.
Hwang, Y., Al-Arabiat, M., & Shin, D.-H. (2016).
Understanding technology acceptance in a mandatory
environment. Information Development, 32(4), 1266–
1283.
Kyakulumbye, S., & Pather, S. (2022). Understanding ICT
adoption amongst SMEs in Uganda: Towards a
participatory design model to enhance technology
diffusion. African Journal of Science, Technology,
Innovation and Development, 14(1), 49–60.
The Role of Culture in User Adoption of Mobile Applications for Self-management of Health: A Conceptual Framework
47

Lai, C., Wang, Q., Li, X., & Hu, X. (2016). The influence
of individual espoused cultural values on self-directed
use of technology for language learning beyond the
classroom. Computers in Human Behavior, 62, 676–
688.
Lee, S. G., Trimi, S., & Kim, C. (2013). The impact of
cultural differences on technology adoption. Journal of
World Business, 48(1), 20–29.
Leidner, & Kayworth. (2006). Review: A Review of
Culture in Information Systems Research: Toward a
Theory of Information Technology Culture Conflict.
MIS Quarterly, 30(2), 357.
Lu, J., Yu, C., Liu, C., & Wei, J. (2017). Comparison of
mobile shopping continuance intention between China
and USA from an espoused cultural perspective.
Computers in Human Behavior, 75, 130–146.
Martins, C., Oliveira, T., & Popovič, A. (2014).
Understanding the Internet banking adoption: A unified
theory of acceptance and use of technology and
perceived risk application. International Journal of
Information Management, 34(1), 1–13.
Masimba, F., Appiah, M., & Zuva, T. (2019). A Review of
Cultural Influence on Technology Acceptance. 2019
International Multidisciplinary Information
Technology and Engineering Conference (IMITEC).
Momani, A., & Jamous, M. (2017). The Evolution of
Technology Acceptance Theories. International
Journal of Contemporary Computer Research (IJCCR),
1(1), 51–58.
Ng, S. I., Lee, J. A., & Soutar, G. (2007). Are Hofstede’s
and Schwartz’s value frameworks congruent?
International Marketing Review, 24(2), 164–180.
Özbilen, P. (2017). The Impact of Natural Culture on New
Technology Adoption by Firms: A Country Level
Analysis. International Journal of Innovation,
Management and Technology, 8(4), 299–305.
Pancar, T., & Ozkan Yildirim, S. (2021). Exploring factors
affecting consumers’ adoption of wearable devices to
track health data. Universal Access in the Information
Society.
Petersen, F., Brown, A., Pather, S., & Tucker, W. D. (2019).
Challenges for the adoption of ICT for diabetes self‐
management in South Africa. The Electronic Journal of
Information Systems in Developing Countries, 86(5),
1–14.
Srite, & Karahanna. (2006). The Role of Espoused National
Cultural Values in Technology Acceptance. MIS
Quarterly, 30(3), 679.
Sriwindono, H., & Yahya, S. (2012). Toward Modeling the
Effects of Cultural Dimension on ICT Acceptance in
Indonesia. Procedia - Social and Behavioral Sciences
,
65(ICIBSoS), 833–838.
Sriwindono, H., & Yahya, S. (2014). The Influence of
Cultural Dimension on ICT Acceptance in Indonesia
Higher Learning Institution. Australian Journal of
Basic and Applied Sciences, 8(5), 215–225.
Straub, D., Keil, M., & Brenner, W. (1997). Testing the
technology acceptance model across cultures: A three
country study. Information & Management, 33(1), 1–
11.
Su, Z., & Sauers, D. A. (2009). The applicability of widely
employed frameworks in cross-cultural management.
Journal of Academic Research in Economics, 1–24.
Sun, S., Lee, P., & Law, R. (2019). Impact of cultural values
on technology acceptance and technology readiness.
International Journal of Hospitality Management, 77,
89–96.
Sun, Y., Wang, N., Guo, X., & Peng, Z. (2013).
Understanding the acceptance of mobile health
services: A comparison and integration of alternative
model. Journal of Electronic Commerce Research,
14(2), 183–201.
Swierad, E., Vartanian, L., & King, M. (2017). The
Influence of Ethnic and Mainstream Cultures on
African Americans’ Health Behaviors: A Qualitative
Study. Behavioral Sciences, 7(4), 49.
Tamilmani, K., Rana, N. P., & Dwivedi, Y. K. (2020).
Consumer Acceptance and Use of Information
Technology: A Meta-Analytic Evaluation of UTAUT2.
Information Systems Frontiers, 1–19.
Tarhini, A., Hone, K., Liu, X., & Tarhini, T. (2017).
Examining the moderating effect of individual-level
cultural values on users’ acceptance of E-learning in
developing countries: a structural equation modeling of
an extended technology acceptance model. Interactive
Learning Environments, 25(3), 306–328.
Teo, T., & Huang, F. (2018). Investigating the influence of
individually espoused cultural values on teachers’
intentions to use educational technologies in Chinese
universities. Interactive Learning Environments, 27(5–
6), 813–829.
Trompenaars, A., & Hampden-Turner, C. (1997). Riding
the Waves of Culture: Understanding Cultural
Diversity in Global Business (2
nd
edition). Nicholas
Brealey.
Ung, S. K. (2017). Role of Cultural and Psychological
Factors Influencing Diabetes Treatment Adherence.
Loma Linda University.
Venkatesh, Thong, & Xu. (2012). Consumer Acceptance
and Use of Information Technology: Extending the
Unified Theory of Acceptance and Use of Technology.
MIS Quarterly, 36(1), 157.
Venkatesh, V., Davis, F., & Morris, M. (2007). Dead Or
Alive? The Development, Trajectory And Future Of
Technology Adoption Research. Journal of the
Association for Information Systems, 8(4), 267–286.
Venkatesh, V., Morris, M. G., Davis, G. B., & Davis, F. D.
(2003). User Acceptance of Information Technology:
Toward a Unified View. MIS Quarterly, 27(3), 425–
478.
Venkatesh, V., Thong, J. Y. L., & Xu, X. (2016). Unified
Theory of Acceptance and Use of Technology: A
Synthesis and the Road Ahead. Journal of the
Association for Information Systems, 17(5), 328–376.
Waki, K., Fujita, H., Uchimura, Y., Omae, K., Aramaki, E.,
Kato, S., Lee, H., Kobayashi, H., Kadowaki, T., & Ohe,
K. (2014). DialBetics. Journal of Diabetes Science and
Technology, 8(2), 209–215.
Yavwa, Y., & Twinomurinzi, H. (2018). Impact of Culture
on E-Government Adoption Using UTAUT: A Case Of
ICT4AWE 2022 - 8th International Conference on Information and Communication Technologies for Ageing Well and e-Health
48
Zambia. 2018 International Conference on
EDemocracy & EGovernment (ICEDEG), April, 356–
360.
Yuan, S., Ma, W., Kanthawala, S., & Peng, W. (2015).
Keep Using My Health Apps: Discover Users’
Perception of Health and Fitness Apps with the
UTAUT2 Model. Telemedicine and E-Health, 21(9),
735–741.
Zhang, Y., Weng, Q., & Zhu, N. (2018). The relationships
between electronic banking adoption and its
antecedents: A meta-analytic study of the role of
national culture. International Journal of Information
Management, 40, 76–87.
Zhao, J., Freeman, B., & Li, M. (2016). Can mobile phone
apps influence people’s health behavior change? An
evidence review. Journal of Medical Internet Research,
18(11).
APPENDIX
Hofstede’s cultural dimensions in relation to diabetes
self-care behaviours
Power
distance
If a DM patient subscribes to a power
distance culture, they may only trust their
doctors or prefer visiting a doctor. The
patient would prefer professional
assistance and advice from a health care
professional rather than using an m-
health a
pp
lication.
Individualism
-collectivism
If a DM patient forms part of an
individualistic society, they will make
their own informed decision as to how to
manage their condition.
If a DM patient who forms part of
collectivistic culture, they will make
health-related decisions based on the
values and beliefs of their societ
y
Masculinity-
femininity
If a DM patient subscribes to a masculine
society, the individual may not self-
manage their condition effectively as
working is a means of survival and
success.
If a DM patient subscribes to a femininity
culture, they will be viewed as nurturers
who care for others. These patients will
make informed health decisions to assist
others in leading healthier lifestyles. This
suggests that they cannot manage their
condition as they must see to the needs of
others.
Uncertainty
avoidance
If a DM patient subscribes to an
uncertainty avoidance society, the
patient may find it difficult to self-
manage their diabetes due to factors such
as crime and the fear of makin
g
an error
which could result in someone obtaining
their
p
ersonal information.
Long-term
orientation-
short-term
orientation
If a DM patient subscribes to a long- term
orientation culture, they will plan their
diabetes self-care activities to ensure
enough finances are available to
maintain their condition.
If a DM patient subscribes to a short-
term orientation culture, the patient will
follow the traditions of their society in
terms of managing their condition.
Indulgence-
Restraint
If a DM patient subscribes to an
indulgence society, they will make
health-related decisions that are
satisfactory to them to ensure that they
are happy.
If a DM patient subscribes to a restraint
culture, they will not take the initiative to
make their own health-related decision
as rules are essential in following a
diabetes self- mana
g
ement re
g
ime.
Trompenaars & Hampden-Turner cultural model in
relation to diabetes self-care behaviour activities
Individualism
versus
Communitari
anism
if a DM patient subscribes to an
“Individualistic culture”, the patient
might be inclined to seek out solutions in
relation to making their own informed
decision and take care of themselves
Universalism
versus
Particularism
If DM patients subscribe to a
“Universalism culture”, the individual
may make diabetes self-care decisions
b
ased on their values and
b
eliefs.
Specific
versus Diffuse
If a DM patient subscribes to a “Specific
culture”, they may share their thoughts
and feelings about their diabetes self-
care activities and decision-making with
others
Affectivity
versus
Neutrality
if a DM patient subscribes to an
“Affective culture”, the patient may
express and share their emotions and
feelings to their doctors about their
diabetes self-care activities
Internal
direction
versus
External
direction
People who form part of an internal
direction culture believe they can control
their environment to achieve their goals.
Achieved
Status versus
Ascribed
Status
If a DM patient subscribes to an ascribed
status, their demographics (race, age and
gender) may influence their diabetes
self-mana
g
ement decision.
Sequential
Time versus
Synchronic
Time
People who form part of a sequential
culture may prefer to have a detailed
agenda of activities and would perform
one activit
y
at a time.
The Role of Culture in User Adoption of Mobile Applications for Self-management of Health: A Conceptual Framework
49
