
A Meta-analytical View on the Acceptance of Mhealth Apps
Luisa Vervier
a
and Martina Ziefle
b
Human Computer Interaction Center, RWTH Aachen University, Campus Boulevard 57, Aachen, Germany
Keywords:
Mhealth Apps, Acceptance, User Diversity, Online Privacy, Trust.
Abstract:
Never before has there been such a driving transformation of healthcare concerning digitalization as in early
2020 due to the pandemic. The digital transformation in the health sector holds great potential to meet the
challenges of demographic change, the financial burden on the health system and the shortage of skilled
workers. One digital solution is the usage of modern information and communication technologies (ICT),
such as mhealth applications (mhealth apps). However, the usage of mhealth apps especially in the German
healthcare system is still evolving and the usage rate of mhealth apps among the population is rather low. To
understand acceptance-relevant factors for the usage, this meta-analytical study presents two samples before
and during pandemic times (survey times 2019 and 2021). To analyse these samples the UTAUT2 acceptance
model in an extended version was applied. The additional factors are online privacy, trust and ehealth literacy.
In total 644 participants took part. The results show, that the factors habit, hedonic motivation, performance
expectancy, social influence and effort expectancy contribute most strongly to the intention to use mhealth
apps as well as the added factor trust. The decisive factor for the user profiles was age.
1 INTRODUCTION
Shortly after the first study in this paper was collected,
the infectious disease SARS-CoV-2 (coronavirus or
COVID-19) spread worldwide. As never before, the
virus has driven digitalization in healthcare. The pan-
demic holds the opportunity to bring forth new ap-
proaches to digitalization in healthcare, which are
currently being developed and applied. Video con-
sultations with doctors, platforms used for clinical
data collection (for example, (climedo, 2020)), dig-
ital help for monitoring COVID-19 and health apps
are some examples of digital applications, that have
gained new prominence. All these telemedicine of-
ferings have given digitalization a new key role in
healthcare, primarily to prevent the spread of infec-
tions. These digital solutions should not only help in
the healthcare sector in the acute phase of the pan-
demic, but also sustainably improve healthcare be-
yond that. The potential of the technical prerequi-
sites (infrastructure, end devices) already exists, but
the widespread use of digital ICT in healthcare is still
far from being achieved. The interlinking of digital
and realistic health services is, in addition to technical
conditions and developments on the part of the health
a
https://orcid.org/0000-0002-9030-6999
b
https://orcid.org/0000-0002-6105-4729
system, also dependent on the acceptance of potential
users.
2 STATE OF THE ART
In the following mhealth apps, acceptance factors and
user diversity is described.
2.1 Mhealth Apps
A trend that has aroused great interest in society in
very recent years is the use of smartphone apps for
self-determined measurement of health parameters.
Maintaining and optimising one’s own health as well
as increasing health awareness contribute to recording
the technical possibilities for measuring vital param-
eters, physical activities as well as exchanging these
data with other users. Despite the wide range of health
apps on the market, usage is low at 14 per cent in
Germany (Meinungsforschungsinstitut, 2019). Most
popular among these apps are sports, nutrition and
weight management apps. Considering that diseases
can be prevented through a healthy lifestyle, plenty
of exercise, a healthy diet and sufficient sleep, it is
beneficial if health-related mhealth apps trigger lively
interest and use among end users. After all, the po-
322
Vervier, L. and Ziefle, M.
A Meta-analytical View on the Acceptance of Mhealth Apps.
DOI: 10.5220/0011088400003188
In Proceedings of the 8th International Conference on Information and Communication Technologies for Ageing Well and e-Health (ICT4AWE 2022), pages 322-329
ISBN: 978-989-758-566-1; ISSN: 2184-4984
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

tential that mhealth apps offer for good healthcare is
very rich. However privacy concerns and usage bar-
riers arise (Powell et al., 2014). mhealth apps are a
highly relevant topic from various perspectives - ei-
ther from a health policy point of view, from a social
point of view or from an economic point of view. The
current state of research still has many research gaps
with regard to user acceptance and user diversity. Es-
pecially in the german-speaking countries, the empir-
ical research on the acceptance of health apps is very
incomplete. For this reason, this study aims to inves-
tigate the user-specific and acceptance-relevant moti-
vations and factors for the use of mhealth offerings
for health maintenance.
2.2 Measuring Acceptance
This study is based on the description of attitudinal
acceptance and considers acceptance in this context
as the willingness to use a health app (technological
innovation). Numerous acceptance models have at-
tempted to map the factors influencing the develop-
ment of acceptance. The majority of current accep-
tance models are based on the Theory of Reasoned Ac-
tion (TRA), postulated by Fishbein and Ajzen (Fish-
bein and Ajzen, 1977). TRA contains basic assump-
tions that were adopted in the development of subse-
quent acceptance models. The theory states that ac-
tual behaviour is the immediate predictor of the use
of a technology in terms of the behavioural or usage
intention. This behavioural intention is in turn de-
termined by the attitude towards the behaviour and
the social norm. In the chronological sequence of
the development stages from the Technology Accep-
tance Model (TAM)1 to TAM3, the Unified Theory of
Acceptance and Use of Technology model (in short:
UTAUT) was developed, which unites the predeces-
sors of the TAMs (Venkatesh and Bala, 2008). The
models were developed with a focus on predicting
adoption in the work context. With the increased use
of technological innovations outside the work context,
the UTAUT and also the UTAUT2 including three ad-
ditional predictors, such as hedonic motivation, mon-
etary value and habit (Venkatesh et al., 2012) cov-
ered a possible model proposal for investigation in the
commercial context or beyond, e.g. the digital health
sector. Therefore, the conceptual basis of the study is
the acceptance model UTAUT2 with its seven factors.
Due to previous studies (Schomakers et al., 2022)
three further constructs were added to the model: (1)
trust in apps, (2) online privacy and (3) ehealth liter-
acy.
2.3 Extension of UTAUT2 Model
The application of the UTAUT2 in the health sector
requires a renewed adaptation. Empirical studies have
shown that specifically when investigating the accep-
tance of mhealth apps, various factors can be both mo-
tive and barrier at the same time and play a decisive
role in the willingness to use them. Trust (Deng et al.,
2018), online privacy (Peng et al., 2016)
and ehealth literacy (Griebel et al., 2018); rep-
resent factors to be considered. Trust is a multidi-
mensional construct that is conceptualised in different
ways depending on the discipline. This paper focuses
on the dimension of technical trust. Trust in technol-
ogy arises from the expected predictability, credibility
and usefulness of the technology (Lippert, 2002). In
the context of health, trust is of relevance since one’
s own health is a valuable resource. People who do
not see health apps as serious and safe support, but
rather a risk to their own health, will not use them. In
the context of ICT, many studies have been conducted
investigating trust in online banking (Luarn and Juo,
2010), eCommerce (Lee et al., 2006) or social media
(Lankton and McKnight, 2011). However regarding
trust in mhealth apps the state of the art is very lim-
ited. Since previous studies have shown that trust is
an important indicator of the intention to use a tech-
nology, it is included in this investigation (Deng et al.,
2018). With the many technical and health benefits of
using mhealth apps, there are factors that work against
using such offerings from the user’s point of view as
e.g. the online privacy attitude. It is a multidimen-
sional construct that can be measured across different
dimensions. For instance, the behaviour of a person,
such as the degree of disclosure of one’s own data on
the Internet, is used to analyse online information pri-
vacy (Acquisti et al., 2015).
Data classified as particularly sensitive may in-
clude, e.g., genetic information, information about
psychological behaviour, illnesses or sexual prefer-
ences (Valentino-Devries, 2010). Especially through
the use of mhealth apps, it is possible to draw conclu-
sions about the person via the phone number (ibid.),
which triggers concerns about social discrimination
among users (Applebaum, 2002). Various studies
confirmed that online privacy is an important factor
for the intention to use digital health offers
(Deng et al., 2018). Therefore it is included in
this study. ehealth literacy - For everyday life, it is
relevant to have a certain ability to deal with one’s
own health and to make conscious decisions about
one’s own health care, disease prevention or even
health promotion. For a long time, the physician,
the pharmacy magazine or even advice from relatives
A Meta-analytical View on the Acceptance of Mhealth Apps
323

and family were the most important source of health
information. With the advent of digital ICT in the
form of ehealth (e.g. platforms) or mhealth apps,
users must have certain digital skills in order to bene-
fit from the offers. The possibility of acquiring health-
relevant knowledge via mhealth apps e.g. can be seen
as an individual and also social opportunity. However,
the great added value of mhealth apps for improving
health care and health care provision, networking and
self-determination of the individual can only be guar-
anteed if the user is able to use them profitably for
himself. ehealth literacy is seen as both a motive and
a barrier for the use of ehealth applications from a
technical and user perspective (Griebel et al., 2018).
The construct of ehealth literacy no longer only de-
scribes the ability to find reliable health information
on the internet but also the handling of interactive dig-
ital health platforms, the use of mhealth apps or the
internet – search for and communication with health
care providers. So far, ehealth literacy as a basic pre-
requisite for the use of ICT in the context of accep-
tance research has only been investigated for ehealth
applications. Studies that examine the construct of
ehealth literacy with regard to the complexity of oper-
ating options of health apps and additionally integrate
the relevant factors into the UTAUT2 model are cur-
rently missing in empirical research. That is why it is
considered in this study.
2.4 User Diversity
A main requirement for the use of mhealth apps is that
they must be operable by different types of users. A
general categorisation of the user group is difficult be-
cause of the diversity that users have in terms of their
age, gender, app experience, health status, etc. The
need to capture the diversity of users is an important
part of understanding the readiness to use mhealth
apps (Peng et al., 2016). Only if users are under-
stood in terms of their diversity it is possible to de-
velop individually tailored solutions and thus achieve
the acceptance of many users. For this reason, socio-
demographic factors such as age, gender, health status
as well as app experience are considered in this study.
3 METHODICAL PROCEDURE
To get insights into users’ attitude towards the usage
of mhealth apps, an online survey was administered
twice to different samples, first in 2019 and secondly
in 2021. Three research questions were leading the
study: (1) Which factors are relevant for the accep-
tance of mhealth apps? (2) Do the extended factors
Figure 1: Overview of meta-analytical study design.
contribute to the prediction of acceptance? and (3)
Which user types or profiles can be formed based on
the socio-demographic factors?
3.1 Study Design
To address the research questions, a meta analysis
was chosen, which statistically analyses data from in-
dependent primary studies that focused on the same
question. The determined effects of the independent
studies are then summarised with the aim of obtain-
ing a more precise estimate of an overall effect (Glass,
1976). Figure 1 gives an overview of all factors which
were included in the meta analysis. Answering the
online survey took about 20 minutes. The question-
naire consisted of three parts. In the first part par-
ticipants were familiarized with the topic of mhealth
apps. Furthermore they were informed, that partici-
pation was voluntary, and not rewarded and that they
could withdraw from the study at any time. In a sec-
ond part, demographic data was assessed. The third
and thus also the main part comprised the acceptance-
relevant factors of the extended UTAUT2 Model. In
the following a detailed description of the empirical
measurements will be outlined.
3.2 Evaluation Measures
In the questionnaire all items had to be evaluated on a
six-point Likert-scale from no agreement at all to to-
tal agreement. Demographic Data. In the first part
the participants’ age, gender, their highest educational
attainment and experience with the use of mhealth
apps was assessed. UTAUT2 Factors. To measure
attitudes towards health apps, items based on Venak-
tesh’s UTAUT2 model (Venkatesh and Davis, 2000)
were partially adopted and adapted to the context in
ICT4AWE 2022 - 8th International Conference on Information and Communication Technologies for Ageing Well and e-Health
324

terms of content. For the performance expectancy
factor, the question was raised to what extent the use
of mhealth apps can have a personal advantage. Ef-
fort expectancy evaluates how much effort the user
has to make using the mhealth apps. Social Influence
includes the social environment of the participant in
the consideration and asks what influence related per-
sons have on the willingness to use a mhealth app.
Facilitating condition measures whether the user has
the necessary resources and assistance available to use
mhealth apps. Hedonic Motivation or rather fun to
use a health app was asked as well as habit which
describes a regular practice with a health app. Finally
the intention to use a health app as a useful application
in everyday life was assessed. In contrast to the orig-
inal UTAUT2 model, actual usage behavior was not
measured, as no usage data was collected as part of
the studies. The price of a mhealth app was also dis-
regarded, as the studies only refer to fictitious health
apps. Online privacy attitude, trust and ehealth liter-
acy were added to the model.
Added Factors to UTAUT2. Attitudes regarding
individual online privacy in the use of mhealth apps
were assessed with the Mobile User’s Concerns for
Information Privacy Scale (MUCIP) from (Xu et al.,
2012). The scale measures the perceived privacy in
dealing with online data and represents a valid mea-
surement instrument, which in the original explicitly
refers to smartphone use. The three dimensions were
surveyed with three items each: (1) perceived surveil-
lance of the user, (2) perceived invasion of privacy and
(3) concerns about secondary use of the data (second
use). In the original, the scale is measured on a seven-
point Likert scale. In order to relate it statistically to
other scales and to avoid the a central tendency as a
response bias, the response format was changed to a
six-point one. Trust in service and technology was
collected as an extended construct for the UTAUT2
model. The items were adapted from K
¨
orber (K
¨
orber,
2018). To measure ehealth literacy the Digital Health
Literacy Index (short: DHLI) according to van der
Vaart (van der Vaart and Drossaert, 2017) was as-
sessed. In the original version, the DHLI measures
operating, search of information and search for infor-
mation skills. The items were reformulated for the
use of mhealth apps to search for health-related infor-
mation.
3.3 Sample Description
The questionnaire was part of a university seminar
and thus participants were recruited from the stu-
dents’ environment via social networks. As can be
seen in table 1 the two samples were very homoge-
nous except of the grade of school education and app
experience. The sample of study I showed a high ed-
ucational degree and a very high app experience (M =
4.64 / max. = 6). In contrast, the sample of study II
had a low level of education and very little work ex-
perience (M = 1.21 / max. = 6). The average age in
study I was around 30 years and in study II around 40
years rounded off. The proportion of women and men
was almost equally distributed. The health status was
averagely high in both samples.
3.4 Statistical Meta-analysis
In order to be methodologically precise and correct,
due to the different samples, a procedure was chosen
that allows each study to be considered as a single
study and still obtain cumulative results. The R pack-
age ”metacor” (Lalibert
´
e et al., 2014) was used as the
statistical evaluation program. The estimation proce-
dure used was the DerSimonian-Laird (DSL) proce-
dure (IntHout et al., 2014). The random-effects model
(RE model) incorporates heterogeneity between stud-
ies by considering the effects as random. The method
uses the correlation coefficients of the individual stud-
ies as effect sizes. These are to be interpreted as con-
fidence intervals and stand as an indicator of signifi-
cance with the p-value.
4 RESULTS
The statistical results for the UTAUT2 factors from
the original model are described first, followed by a
summary of the extended factors as well as the de-
scription of a user profile based on the samples. Sig-
nificance level of the correlations range from * =
p<.05, ** = p< .01 to *** = p <.001.
UTAUT2 Factors. In the meta analysis, only
one significant difference between the individual
UTAUT2 constructs could be found. The factor fa-
cilitating condition differed statistically significant (r
= .135 (.230, .037) p = 0.003) which implies that
necessary resources and assistance availability to use
mhealth apps has changed. All other factors do not
show any statistically significant variability and can
be concluded as homogeneous. This means that the
constructs of the different studies can be summarised
and be seen as stable and explainable acceptance fac-
tors. The highest influence on the intention to use
health apps was: (1) habit (r = .787 (.815, .756), p
= n.s.), (2) hedonic motivation (r = .670 (.710, .625),
p = n.s.), (3) performance expectancy (r = ,636 (.695,
.569), p = n.s.),(4) social influence (r = .390 (.510,
.255), p = n.s.), (5) effort expectancy (r = .361 (.412,
A Meta-analytical View on the Acceptance of Mhealth Apps
325
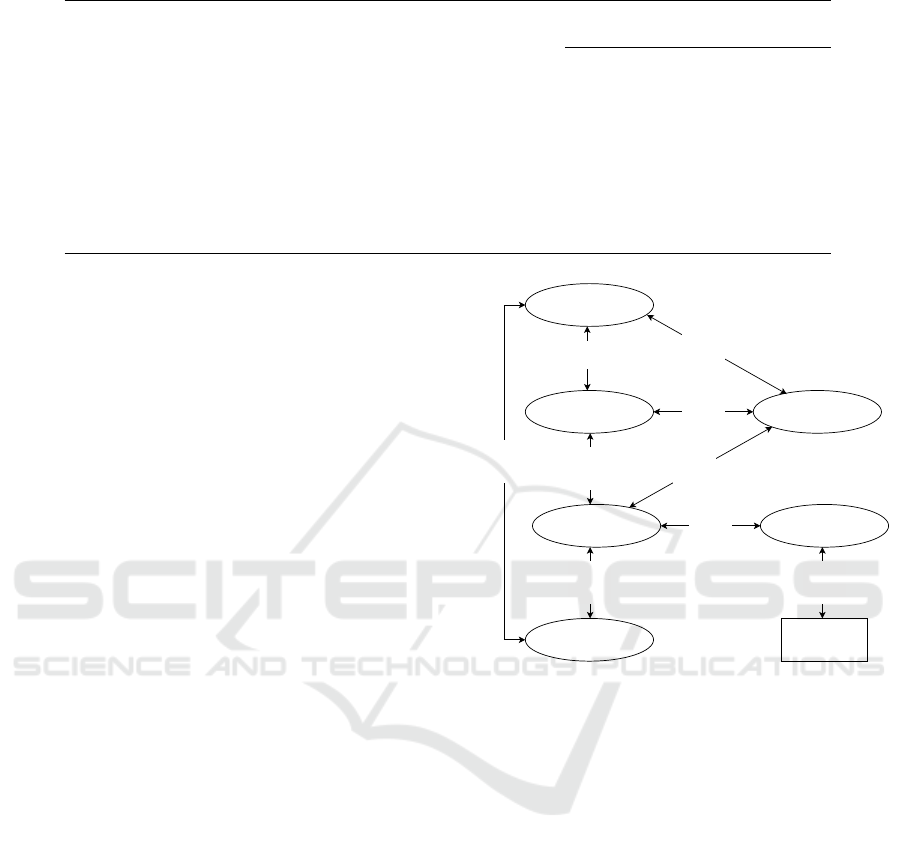
Table 1: Demographic data of study I and II separated by collection time.
study I 2019 study II 2021
n = 278 n = 366
age [years] M (SD) 29.98 (14.39) 37.90 (18.67)
sex women 57% 60%
men 43% 40%
education no certificate 1% 31%
certificate of secondary education 5% 35%
general certificate of secondary education 7% 8%
general qualification for university degree 87% 26%
health status 4.49 (.92) 4.28 (1.07)
app experience 4.64 (.89) 1.21 (.48)
.276), p = n.s.) and finally (6) faciliating condition (r
= .135 (.230, .037), p = .003).
In Study I, the habit and usage intention had the
highest relationship (r = .804**), followed by the rela-
tionship between performance expectancy and hedo-
nic motivation (r = .715**), hedonic motivation and
usage intention (r = .677**), and the relationship be-
tween hedonic motivation and habit (r = .600**) as
well as between performance expectancy and usage
intention (r = .600**). Study II showed also the high-
est correlation between habit and usage intention (r
= .775**), followed by hedonic motivation and per-
formance expectancy (r = .704**), usage intention
and hedonic motivation (r = .665**), usage intention
and performance expectancy (r = .665**) and faciliat-
ing condition and effort expectancy (r = .662**). All
other correlations from study I and II were moderate
and can be found in table 2.
Impact of Extended Factors on Intention to
Use. Perceived online privacy, ehealth literacy and
trust were included in the meta analysis as compa-
rable extended constructs. The correlations between
the extended factors were not statistically significant.
Thus, the results in the individual studies can be sum-
marised. Trust had the strongest positive influence on
intention to use (r = .577 (.639, .508), p = n.s.).
All other correlations were negative, meaning
the higher the perceived invasion (r = -.215 (-
.110, −.315), p = n.s.), the concern of secondary use (r
= -.189 (-.113, -.263), p = n.s.), the perceived surveil-
lance (r = -.186 (-.111, -260), p = n.s.) and the ehealth
literacy competence (r = -.037 (.204, -.274), p = n.s.),
the lower the intention to use a smartphone with a
mhealth app.
Impact of Socio-deomgraphic Data Among
Each Other and on Intention to Use. Figure 2
shows the significant relationships between socio-
demographic data and the intention to use. For a bet-
ter overview, only the significant relationships have
been included in the graph and non-significant ones
have been omitted. The variables are each connected
usage
intention
-.267**
(n = 684)
sex
-.106*
(n = 693)
training degree
school certificate
.137**
(n = 688)
age health status
-.372**
(n = 679)
.137*
(n = 688)
mhealth app
experience
-.271**
(n = 688)
.129**
(n = 651)
.532**
(n = 688)
-.127*
(n = 481)
Figure 2: Overview of meta-analytical study design.
with arrows on which the positive or negative correla-
tion is shown by indicating the correlation coefficient,
together with the sample size from which the signif-
icant effect results. Regarding age, older participants
were found to have a lower health status (r = -.372**)
as well as a lower experience with apps (r = -.271**)
in contrast to youngers. However, older participants
showed a higher training degree (r = -.132**) in com-
parison with younger participants. Significant influ-
ences of the user factor sex was found. Women re-
ported to be willing to use a mhealth app more often
than men (r = -.127*). Moreover, they had a lower
training degree than men (r = -.106*). Another sta-
tistically significant correlation was found within the
app experience. The more experienced the partic-
ipants considered themselves to be in dealing with
apps, the better their health status (r = .129**) and
the better their education (r = .532**).
ICT4AWE 2022 - 8th International Conference on Information and Communication Technologies for Ageing Well and e-Health
326

Table 2: Correlation between UTAUT2-factors (PE = performance expectancy, EE = effort expectancy, SI = social influence,
FC = faciliating condition, HM = hedonic motivation, UI = usage intention). Upper correlations in bold refer to study I, lower
correlations in italics refer to study II.
UTAUT2 factors PE EE SI FC HM H UI
PE 1 .438** .320** .280** .715** .551** .600**
EE .349** 1 -.047 .510** .371** .226** .365**
SI .358** -.084 1 -.150* ,376** .512** .456**
FC .235** .662** -.152** 1 .201** -.058 -.081
HM .704** .428** .332** .293** 1 .600** .677*
H .599** .205** .444** .098 .569** 1 .804**
UI .665** .332** .326** .180** .665** .775** 1
5 DISCUSSION
The meta-analysis’ aim was to aggregate the results
of the two studies conducted and to examine them
with regard to acceptance-relevant factors. It was
found that five factors were prominent in measuring
mhealth app acceptance: habit, hedonic motivation,
performance expectancy, social influence and effort
expectancy. The strongest influence on the inten-
tion to use was found with the factor habit. Due to
the fact that the use of smartphones with integrated
apps is familiar to the sample studied, it has become
a self-evident process (M
¨
oller, 2016). Habit is un-
derstood as an action once learned that runs auto-
matically without conscious control (Stangl, 2018).
Thus, the functions of the app corresponds to the ha-
bitual actions performed when using a health app.
As a recommendation for mhealth app developers it
can be maintained that the operation of the app must
be simple and include the usual interaction gestures
(touch gestures) when using the smartphone. Hedo-
nic motivation was the second most important fac-
tor. This result was already reflected in the state of re-
search on the use of health apps in other studies (Peng
et al., 2016). In order to achieve a high usage rate
of health apps, playful elements must be included in
the app that motivate and give pleasure. Playful so-
lutions in the form of gamification or augmented re-
ality (computer-supported reality approaches) are ap-
proaches that should be incorporated in the develop-
ment of health apps. Scientific results on the success
of integrating playful approaches to promote health
already exist (Schlomann et al., 2019), and can serve
as orientation. The third most important factor was
performance expectancy. This result is in line with
other studies on health app acceptance research (Alam
et al., 2020). The performance expectation reflects
the utility of the app in terms of fitness apps, monitor-
ing a health situation, managing and controlling cer-
tain health conditions. As a recommendation it can
be stated that the app must have appropriate techni-
cal functions that enable the monitoring, management
and control of fitness or a disease. The app’s perfor-
mance (e.g. measuring vital parameters) must be of
a high standard. Social influence was ranked fourth
most important. It refers to the degree to which peo-
ple perceive that others they care about believe they
should use a health app. Using a health app strength-
ens the ability to connect with other users they con-
sider important. The ability to share data about per-
sonal fitness levels with other fitness app users is an
important aspect of maintaining motivation that must
be further considered in technical development. Ef-
fort expectancy was the last influencing factor and
describes how much effort the user has to make us-
ing the app. Therefore, one recommendation could
be that the app should obtain a simple and easy-to-
follow menu structure. Facilitating condition was
the only factor that differed in the meta analysis. It
describes the knowledge of how to use a mhealth app.
Since the sample of study II did not bring a lot of app
experience, this factor was not homogenous with the
other result. The second research question focused on
the added UTAUT2 factors to measure the intention
to use. Trust contributed strongly to the intention to
use. The state of research on the influence of trust
on intention to use could be proven with this study.
One recommendation that emerges from the results is
that mhealth app providers must transparently explain
quality aspects and trustworthiness. This includes in-
formation about the possibilities of the app as well as
the risks and limitations. The influence of online pri-
vacy on intention to use had been confirmed in this
study
(Deng et al., 2018). Concerns about data theft
or sharing the information with third parties were
particularly high for health-related data Thus, it can
be recommended that the protection of privacy must
be guaranteed by technical data protection measures.
Users must decide for themselves if and with whom
they want to share data. Studies related to eHealth so-
lutions have already shown that the higher the digital
A Meta-analytical View on the Acceptance of Mhealth Apps
327

skills and knowledge of understanding and processing
health-related information, the higher the willingness
to use it(Griebel et al., 2018).
Based on the results of this study no statistically
effect could be observed for mHealth apps. The third
research question focused on which user groups can
be formed on the basis of socio-deomgraphic data.
Thus, in this work, a user group was determined in
terms of content on the basis of the positive correla-
tions between two variables, and conversely, another
user group from the negative correlations. The fol-
lowing different characteristics emerged: one group
consists of young, low-educated, however healthy and
app-experienced participants who are willing to use
health apps. The other group consists of older par-
ticipants with good health, little experience in using
mhealth apps however with a higher educational at-
tainment. This group has a low intention to use apps.
Both groups differ significantly from each other. Age
is to be regarded as the decisive factor that influences
all other factors. The older the participants, the less
experience they have in using apps (Searcy et al.,
2019) and expertise in using digital ICT in the health
sector
(van der Vaart and Drossaert, 2017), which are rel-
evant for the acceptance of health apps. Due to their
diversity, the different types of users require techni-
cal and content solutions that are specially adapted to
them and contribute to increasing acceptance.
6 LIMITATION AND OUTLOOK
The findings from the present study have provided in-
sights into acceptance-relevant factors regarding the
intention to use mhealth apps. However, the context
of our study was limited. First of all the study was
mainly conducted in the students surrounding at uni-
versity which resulted in a rather young sample. Even
though results could be detected for exactly this type
of user group, further studies should focus on broader
samples to present a representative whole. Moreover,
this study only evaluated an associated mhealth app.
In order to receive real data in terms of hand-on-
experience, it is necessary to develop a mhealth app
with different features and evaluate the usability with
regard to acceptance-relevant factors. Furthermore,
the app area of mhealth apps is divers and include
all health care areas from information, prevention,
care of complaints or also products, self-management,
therapy, rehabilitation in the form of aftercare and
monitoring. Further studies should consider the dif-
ferent fields and include them in acceptance studies.
The ability to operate a mhealth app is a basic pre-
requisite for the willingness to use it. The acceptance
of mhealth apps must also be investigated on people
who are ill, as otherwise there is an overestimation
of the capability and an underestimation of the actual
needs. In addition, research activities should be inves-
tigated with regard to the needs and requirements of
mhealth apps on behalf of limited users who require
barrier-free access due to their physical, mental or
even cognitive condition. It is important to understand
how the requirements of healthy people for the de-
sign of mhealth apps differ from those of people with
poorer health, in order to develop mhealth solutions
that can be adequately tailored to the corresponding
user groups. Due to lack of evidence so far on the
effectiveness specifically with regard to care and ther-
apeutic apps (Payne et al., 2015), further long-term
studies are needed.
ACKNOWLEDGEMENTS
The authors thank all participants for sharing their
thoughts and opinions. We would also like to thank
the reviewers for their valuable feedback.
REFERENCES
Acquisti, A., Brandimarte, L., and Loewenstein, G. (2015).
Privacy and human behavior in the age of information.
Science, 347(6221):509–514.
Alam, M. Z., Hoque, M. R., Hu, W., and Barua, Z.
(2020). Factors influencing the adoption of mhealth
services in a developing country: A patient-centric
study. International Journal of Information Manage-
ment, 50:128–143.
Applebaum, P. (2002). Privacy in psychiatric treatment:
threats and response. American Journal of Psychia-
try, 159(11):1809–1818.
climedo (2020). climedo. available online under https:
//climedo.de/ last checked on 01.20.2022.
Deng, Z., Hong, Z., Ren, C., Zhang, W., and Xiang, F.
(2018). What predicts patients’ adoption intention to-
ward mhealth services in china: empirical study. JMIR
mHealth and uHealth, 6(8):e172.
Fishbein, M. and Ajzen, I. (1977). Belief, attitude, inten-
tion, and behavior: An introduction to theory and re-
search.
Glass, G. V. (1976). Primary, secondary, and meta-analysis
of research. Educational researcher, 5(10):3–8.
Griebel, L., Enwald, H., Gilstad, H., Pohl, A.-L., More-
land, J., and Sedlmayr, M. (2018). ehealth literacy re-
search—quo vadis? Informatics for Health and Social
Care, 43(4):427–442.
IntHout, J., Ioannidis, J. P., and Borm, G. F. (2014).
The hartung-knapp-sidik-jonkman method for ran-
dom effects meta-analysis is straightforward and
ICT4AWE 2022 - 8th International Conference on Information and Communication Technologies for Ageing Well and e-Health
328

considerably outperforms the standard dersimonian-
laird method. BMC medical research methodology,
14(1):25.
K
¨
orber, M. (2018). Theoretical considerations and devel-
opment of a questionnaire to measure trust in automa-
tion. In Congress of the International Ergonomics As-
sociation, pages 13–30. Springer.
Lalibert
´
e, E., Legendre, P., Shipley, B., and Lalibert
´
e, M. E.
(2014). Package ‘fd’. Measuring functional diver-
sity from multiple traits, and other tools for functional
ecology.
Lankton, N. K. and McKnight, D. H. (2011). What does
it mean to trust facebook? examining technology and
interpersonal trust beliefs. ACM SIGMIS Database:
the DATABASE for Advances in Information Systems,
42(2):32–54.
Lee, H. Y., Ahn, H., and Han, I. (2006). Analysis of
trust in the e-commerce adoption. In Proceedings of
the 39th Annual Hawaii International Conference on
System Sciences (HICSS’06), volume 6, pages 113c–
113c. IEEE.
Lippert, S. K. (2002). An exploratory study into the rel-
evance of trust in the context of information systems
technology.
Luarn, P. and Juo, W.-J. (2010). The role of trust in technol-
ogy within the tam in the context of nfc mobile pay-
ment. Journal of Information and Optimization Sci-
ences, 31(4):875–896.
Meinungsforschungsinstitut, S. (2019). Internetsuche zum
thema gesundheit. Online verf
¨
ugbar unter https://de.
statista.com/statistik/daten/studie/163487/ umfrage/
internetnutzung-bei-der-informationssuche-zum\
\-thema-gesundheit/ Zuletzt gepr
¨
uft am 20.10.2020,
2(2017).
M
¨
oller, R. (2016). Das smartphone als leitmedium. In Ent-
Grenztes Heranwachsen, pages 185–199. Springer.
Payne, H. E., Lister, C., West, J. H., and Bernhardt, J. M.
(2015). Behavioral functionality of mobile apps in
health interventions: a systematic review of the litera-
ture. JMIR mHealth and uHealth, 3(1):e20.
Peng, W., Kanthawala, S., Yuan, S., and Hussain, S. A.
(2016). A qualitative study of user perceptions of mo-
bile health apps. BMC Public Health, 16(1):1158.
Powell, A. C., Landman, A. B., and Bates, D. W. (2014). In
search of a few good apps. Jama, 311(18):1851–1852.
Schlomann, A., Rasche, P., Seifert, A., Sch
¨
afer, K., Wille,
M., Br
¨
ohl, C., Theis, S., and Mertens, A. (2019).
Augmented reality games for health promotion in old
age. In Augmented Reality Games II, pages 159–177.
Springer.
Schomakers, E.-M., Lidynia, C., Vervier, L. S., Valdez,
A. C., Ziefle, M., et al. (2022). Applying an extended
utaut2 model to explain user acceptance of lifestyle
and therapy mobile health apps: Survey study. JMIR
mHealth and uHealth, 10(1):e27095.
Searcy, R. P., Summapund, J., Estrin, D., Pollak, J. P.,
Schoenthaler, A., Troxel, A. B., and Dodson, J. A.
(2019). Mobile health technologies for older adults
with cardiovascular disease: Current evidence and fu-
ture directions. Current Geriatrics Reports, 8(1):31–
42.
Stangl, W. (2018). Online lexikon f
¨
ur psycholo-
gie und p
¨
adagogik. Online verf
¨
ugbar unter:
http://lexikon.stangl.eu/7024/manipulation/[letzter
Zugriff: 14. 08. 2018].
Valentino-Devries, J. (2010). Unique phone id numbers ex-
plained. The Wall Street Journal.
van der Vaart, R. and Drossaert, C. (2017). Development
of the digital health literacy instrument: measuring
a broad spectrum of health 1.0 and health 2.0 skills.
Journal of medical Internet research, 19(1):e27.
Venkatesh, V. and Bala, H. (2008). Technology acceptance
model 3 and a research agenda on interventions. De-
cision sciences, 39(2):273–315.
Venkatesh, V. and Davis, F. D. (2000). A theoretical exten-
sion of the technology acceptance model: Four longi-
tudinal field studies. Management science, 46(2):186–
204.
Venkatesh, V., Thong, J. Y., and Xu, X. (2012). Consumer
acceptance and use of information technology: ex-
tending the unified theory of acceptance and use of
technology. MIS quarterly, pages 157–178.
Xu, H., Gupta, S., Rosson, M. B., and Carroll, J. M. (2012).
Measuring mobile users’ concerns for information pri-
vacy.
A Meta-analytical View on the Acceptance of Mhealth Apps
329
