
Acute Myocardial Infarction and Related Drugs
Jianing Zhong
School of Chemistry, The University of Nottingham, Nottingham, NG7 2RD, U.K.
Keywords:
Acute Myocardial Infarction, Aspirin, Clopidogrel.
Abstract:
As the medical name for a heart attack, acute myocardial infarction (AMI) is a common disease with serious
symptoms and no relevant targeted drugs. Extremely critical consequences of AMI in mortality, morbidity,
and cost to the society have been the great challenge in the long-term development of human society. In
addition, the advent of AMI and results of clinical trials on therapy have major implications from the
epidemiological, societal, and patient points of view. Hence, it is of great significance to develop drugs related
to acute myocardial infarction with excellent pharmacokinetics. This paper discusses the pathophysiology,
evolving drugs on therapy of acute myocardial infarction and incorporates the chemical structure,
pharmacology, underlying economics of pertinent drugs and further discussion of the drugs related to the
AMI.
1 INTRODUCTION
1.1 Definition and Categories
Acute myocardial infarction, commonly defined as
myocardial necrosis due to acute, persistent ischemia
and hypoxia of the coronary arteries; Also known as
a sudden heart attack, it is a life-threatening condition
that occurs when blood flow to the heart muscle is
suddenly interrupted, leading to tissue damage
(White, Chew, 2008). Furthermore, a new definition
of myocardial infarction has been consensus group
put forward in 2000 from the European Society of
Cardiology and the American College of Cardiology,
with the definition being based on myocyte necrosis
as determined by troponins in the clinical setting of
ischemia (White, Chew, 2008).
Acute myocardial infarction is a major cause of
morbidity and mortality worldwide, with two
entities. According to the difference between ST
segment elevation and non-elevation on
electrocardiogram, acute myocardial infarction can
be classified as ST segment elevation myocardial
infarction (STEMI) and non-ST segment elevation
myocardial infarction (NSTEMI) (Boersma, 2003).
In addition to distinguishing from by ST segment, the
two types of acute myocardial infarction can also be
clinically distinguished by coronary angiographic
findings (Most of the coronary arteries in NSTEMI
are not completely occluded).
1.2 Factors and Symptoms
Acute myocardial infarction can be caused by several
factors, such as age, genetics. However, extreme
lifestyles may be the biggest culprit. Epidemiological
studies have highlighted the role of lifestyle factors
in acute myocardial infarction. Poor lifestyle habits,
such as obesity and alcohol abuse, can potentially put
people at risk for acute myocardial infarction. While
chest pain and shortness of breath are typical
symptoms of an acute myocardial infarction, there
are several different symptoms, including nausea,
anxiety, or dizziness (Boersma, 2003).
1.3 The Number of Cases in China and
Other Countries
According to incomplete statistics, there are 3
million people suffer from STEMI each year, and
there are also more than 4 million cases of NTSEMI
(White, Chew, 2008). Acute myocardial infarction, a
common disease in developed countries, affects
more than 1 million people in the United States each
year. However, acute myocardial infarction is also on
the rise trend in developing countries at present. For
example, acute myocardial infarction has become a
major cause of hospitalization and mortality in
China. According to incomplete statistics, there are
approximately 4 million cases of acute myocardial
infarction in China (White, Chew, 2008).
574
Zhong, J.
Acute Myocardial Infarction and Related Drugs.
DOI: 10.5220/0011238600003443
In Proceedings of the 4th International Conference on Biomedical Engineering and Bioinformatics (ICBEB 2022), pages 574-578
ISBN: 978-989-758-595-1
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
1.4 Drugs Used to Treat the Disease
As the main potential incentive of acute myocardial
infarction, platelet hypperaggregation is constantly
devouring human life. Based on extensive
pharmacological evidence, antithrombotic
medications such as Aspirin and Clopidogrel are the
most potentially effective antiplatelet agents
contribute to treat platelet hypperaggregation. In
addition, Nitrates and Stains as other first-lines
medicine are adopted in improving the long-term
outlook in survivors of the acute phase. Although, the
majority of pharmacological evidence are based on
the clinal trials from patients with STEMI, the first-
lines medicine also available optional for the
NSTEMI patients (Boersma, 2003). In this paper,
Aspirin and Clopidogrel are discussed in the next
stages as the main treatment agents for acute
myocardial infarction in the article.
2 DESCRIPTION OF CHEMICAL
STRUCTURE OF DRUGS
In the description, the structures for aspirin and
clopidogrel are shown by two figures. In addition,
there are two more figures of the chemistry
properties for aspirin and clopidogrel.
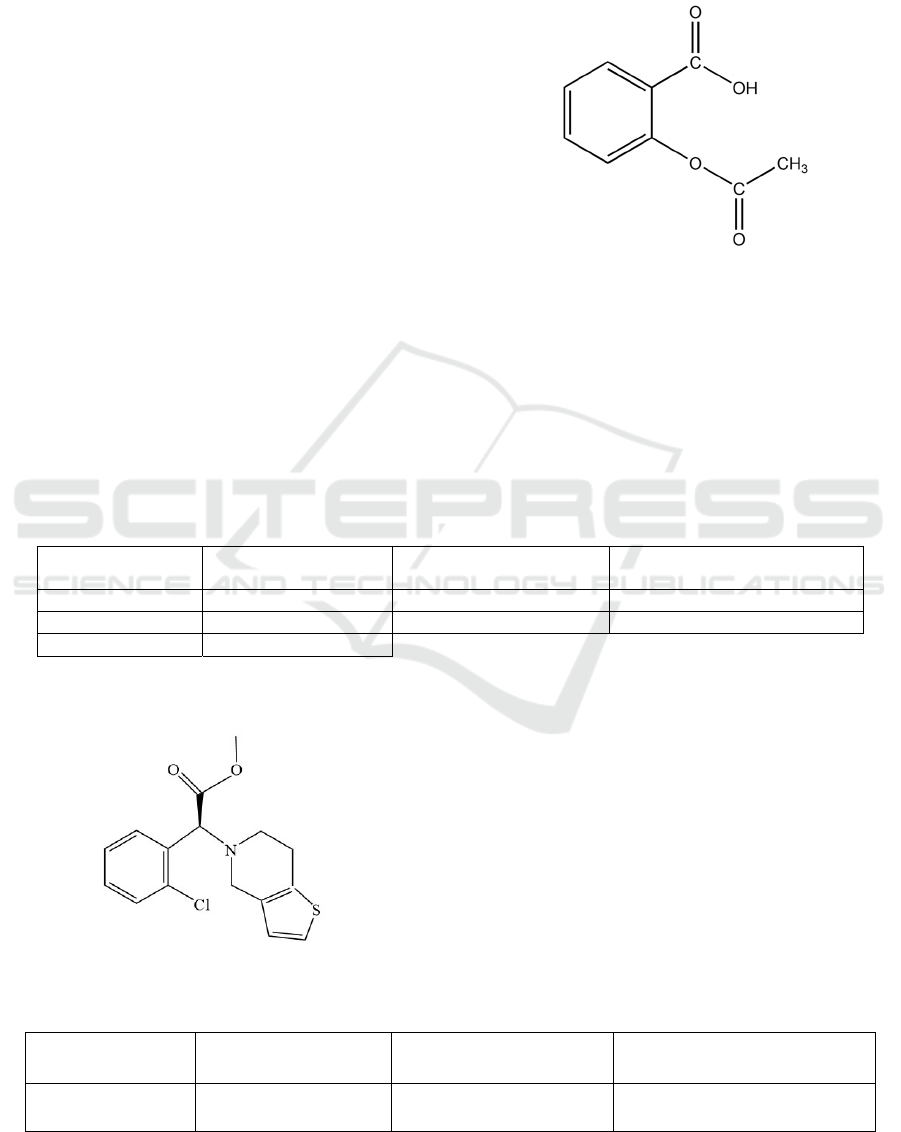
2.1 Aspirin
Figure 1: the structure of aspirin
As known as acetylsalicylic acid, with the IUPAC
name 2-Acetoxybenzoic acid, is a salicylic acid class
of drugs. As a white crystalline or crystalline powder,
odorless or with a slight odor of acetic acid, slightly
soluble in water, soluble in ethanol, soluble in ether
and chloroform, and acidic in aqueous solutions. The
structure of aspirin and the properties of Aspirin can
be demonstrated as Figure 1 and Table 1:
Table 1: the properties of Aspirin
Formula
𝐶
𝐻
𝑂
Boiling point
321.4°C at 760 mmHg
Molar mass
180.16
Solubility in wate
r
3.3𝑔/𝐿
Density
1.35𝑔 𝑐𝑚
Vapor pressure
0.000124𝑚𝑚𝐻𝑔 𝑎𝑡 25°𝐶
Boiling Point
136 140℃
2.2 Clopidogrel
Figure 2: The structure of 𝑐𝑙𝑜𝑝𝑖𝑑𝑜𝑔𝑟𝑒𝑙.
As known as a drug that inhibits platelet
aggregation, with the IUPAC name (+) − (𝑆) −
𝑚𝑒𝑡h𝑦𝑙 2 − (2 − 𝑐h𝑙𝑜𝑟𝑜𝑝h𝑒𝑛𝑦𝑙) − 2 − (6,7 −
𝑑𝑖h𝑦𝑑𝑟𝑜𝑡h𝑖𝑒𝑛𝑜[3,2 −𝑐]𝑝𝑦𝑟𝑖𝑑𝑖𝑛 − 5(4𝐻) −
𝑦𝑙)𝑎𝑐𝑒𝑡𝑎𝑡𝑒 (J.-M. Pereillo, 2002). The structure of
clopidogrel and the properties of Aspirin can be
demonstrated as Figure 2 and Table 2:
Table 2: The properties of Clopidogrel
Formula
𝐶
𝐻
𝐶𝑙𝑁𝑂
𝑆
Boiling point
423.7°C at 760 mmHg
Molar mass
321.86
Density
1.32𝑔 𝑐𝑚
Acute Myocardial Infarction and Related Drugs
575
3 DISCUSSION OF DRUG
PHARMACOLOGY
In the discussion of pharmaceutical pharmacology,
aspirin and clopidogrel would be discussed in three
separate parts, which are pharmacodynamics,
Pharmacokinetics, and the Mode of Delivery.
3.1 Aspirin
3.1.1
Pharmacodynamics
As one of the earliest antiplatelet drugs, aspirin was
synthesized in the late 19th century, and its
antiplatelet action was discovered British
pharmacologist John Robert Vane in 1970s.
As an antithrombotic drug, aspirin is an inhibitor
of cyclooxygenase (COX) (Warner, 2002). The
irreversible acetylation of aspirin with
cyclooxygenase leads to the inactivation of COX,
which in turn disables the pathway of thromboxane
formation and ultimately prevents high platelet
aggregation. (The main involved in antithrombotic is
COX-1 (Warner, 2002). Studies have shown that
COX-2 plays a significant role in prostaglandin
production.)
3.1.2
Pharmacokinetics
As a weak acid, aspirin dissociates very slight in the
stomach. As a result, aspirin is quickly absorbed by
cell membranes in the stomach. Nevertheless, in the
small intestine, as the PH value gradually increases,
the amount absorbed gradually decreases.
According to long-term clinical trials, only 20 to
50 percent of aspirin is ionized; the rest is absorbed
into the bloodstream. Aspirin has a half-life of two to
three hours (Bond, 2007). For example, the half-life
of a single dose of 0.65g aspirin in breast milk is about
3.8 to 12.5 hours. (Because aspirin is excreted in
breast milk, large doses can have an adverse effect on
infants.)
3.1.3
Mode of Delivery
Aspirin is mainly taken orally. The daily dose needs
to be determined according to the stage of the disease
and the patient's constitution. Generally, small doses
are given priority to, usually 50 to 150mg per day
(Bond, 2007). However, during an acute myocardial
infarction, 325 mg of aspirin can be taken orally for
the first time, and then 100 mg a day (Ferguson,
1970).
3.2 Clopidogrel
3.2.1
Pharmacodynamics
As one kind of antithrombotic agent, clopidogrel is a
P2Y12 purine receptor antagonist (Mega, 2009).
P2Y12 receptor plays an important role in mediating
the sustained activation of stimulated by ADP, and is
a major receptor that mediates platelet adhesion.
P2Y12 receptor antagonist can inhibit the activation
and amplification of platelet induced by ADP and
produce effective antithrombotic effect.
3.2.2
Pharmacokinetics
As a prodrug, clopidogrel in activated in two steps by
two enzymes. The enzyme in first step mainly is
CYP2C19 (Mega, 2009). There are many different
enzymes involved in the second step (Hydrolysis
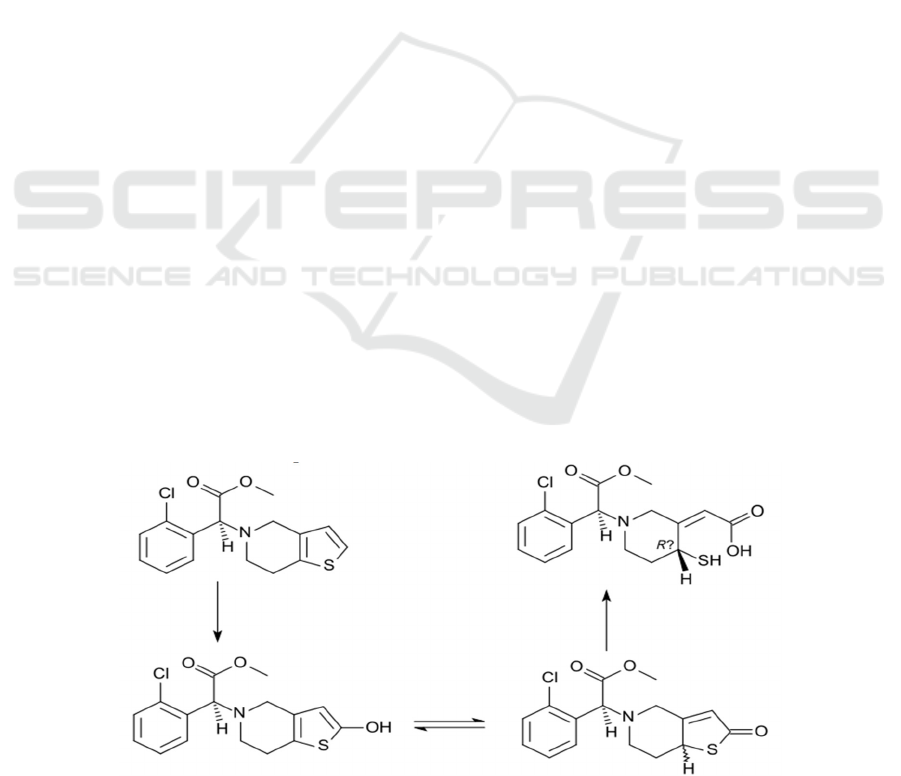
reaction), such as CYP2C19, CYP2C9. The figure 3
briefly describe the progress of pharmacokinetics for
clopidogrel.
Figure 3: the progress of pharmacokinetics for clopidogrel. The primarily step is oxidation with CYP2C19 enzyme as catalyst.
The two structures at bottom are tautomer. Moreover, the second step is reaction of hydrolysis.
ICBEB 2022 - The International Conference on Biomedical Engineering and Bioinformatics
576

Specifically, clopidogrel was not effective in
treating acute myocardial infarction for about 2 hours
after oral administration, since clopidogrel itself is
not effective in inhibiting platelets. However, after
being activated by cytochrome P450 enzyme
(CYP2C19) in liver, clopidogrel structure is
destroyed (thiophene ring is opened), resulting in the
formation of new substances that can fight
thrombosis (Simon, 2009). The entire clopidogrel is
digested in the human body, and it takes about 3.5 to
4.5 hours for the drug to take effect and wear off.
3.2.3 Mode of Delivery
Clopidogrel was mainly taken orally once a day and
can be taken for a long time. Dosages vary from
50mg to 150mg, depending on age (best taken after
meals). For rapid action, clopidogrel can also be
taken orally in 300 to 600mg doses at a time (Collet,
2009).
4 DISCUSSION OF DRUG
ECONOMICS
In order to discuss the drug Economics, the cost and
the number of prescription and sales of aspirin and
clopidogrel are briefly shown.
4.1 Aspirin
According to Clinical (2018), aspirin prescription
costed around $4.48 in the United States and as little
as £1.28 in the UK. It proves that aspirin is within the
reach of almost everyone. Meanwhile, In the United
States, there are more than five million patients who
need aspirin and a staggering 19 million aspirin
prescriptions (Boersma, 2003).
4.2 Clopidogrel
Clinical (2017) stated that nearly all clopidogrel is
covered by most Medicare and insurance plans and
each patient effectively treats acute myocardial
infarction for about $10 per month (Boersma, 2003).
In 2018, this is projected to be more than 4 million
AMI patients in America and number of
prescriptions in the United States is exceeding 20
million.
In a word, the low cost of aspirin and Clopidogrel
is an appropriate guarantee for acute myocardial
infarction. At the same time, the large number of
patients and prescriptions suggests that there still be
a large market and a sound momentum of growth for
them.
5 FURTHER DISCUSSION
As same as the other drugs, clopidogrel and aspirin
own side effects as well. In the further discussion,
both adverse effects are discussed and other types of
antithrombotic drugs for acute myocardial infarction
is briefly covered as well.
5.1 Aspirin
Serious side effect associated with aspirin treatment
include:
Gastrointestinal reaction. Oral aspirin can
directly affect the stimulation of gastric mucosa and
cause nausea and vomiting, and long-term use will
lead to gastritis membrane damage and gastric ulcer
and gastric bleeding and other symptoms
(Vishweshwar, 2005).
Allergic reaction to aspirin. Aspirin can cause
rashes, angioedema, asthma, and other allergic
reactions in allergic people.
Aspirin may also influence the central nervous
system. Generally, when taking a large dose, there
will be headaches, vertigo, tinnitus and other
symptoms, and there will be coma and other
symptoms when taking too much.
Liver and kidney damage. Side effects of aspirin
include toxicity to the liver and kidneys. Aspirin is
broken down in the liver and then excreted through
the kidneys, resulting in decreased liver and kidney
function.
5.2 Clopidogrel
As an inhibitor of platelets, clopidogrel affects the
lifespan of platelets by irreversibly changing the
ADP receptor of platelets, leading to
thrombocytopenia, and the lack of platelets is the
culprit of the bleeding. Therefore, the main side
effect is bleeding, such as subcutaneous bleeding,
gingival bleeding. Side effects includes
gastrointestinal reactions, allergies, liver and kidney
dysfunction, and leukopenia are usual in clinical
treatment as well (Diener, 2004).
Platelet membrane glycoprotein IIb/IIIa
(GPIIb/IIIa) receptor antagonists are also
antithrombotic agents (GPIIb/IIIa antagonists are
ligand mimics that prevent fibrinogen from binding
to activated platelets, thereby directly inhibiting
platelet aggregation) (Kaufman, 1972). Three drugs
Acute Myocardial Infarction and Related Drugs
577

are currently on the market: tirofiban, a small non-
peptide molecule that mimics fibrinogen binding
sites; Etibateptide, a cyclic heptapeptide with a
lysine-glycine-aspartic acid (KGD) sequence, also
mimics the fibrinogen binding sequence in
GPIIb/IIIa; And accimab, a humanized antigen-
binding fragment of a murine monoclonal antibody
(Simon, 2009).
6 CONCLUSION
This article provides a brief overview to acute
myocardial infarction from the perspective of its
definition and introduces two drugs for the
prevention and treatment of AMI from an
antithrombotic perspective——aspirin and 1.
chemical structure, and corresponding chemical
properties of these two drugs are described in detail
in the follow section. Furthermore, through the parts
of pharmacodynamics and pharmacokinetics, the
pharmacology of these two drugs is referred at
length.
However, these two drugs also own assignable
underlying adverse effects. Unfortunately, there is
still no specific drug to treat or prevent acute
myocardial infarction. These two points are cursorily
discussed likewise in further discussion.
Overall, as a common cardiovascular disease,
acute myocardial infarction owns a higher mortality
rate than the parallel diseases. Nevertheless, due to
the understanding of its pathogenesis and the timely
investment of related drugs, it has declined
significantly in the past decades. On the contrary,
both number and the age range of the acute
myocardial infarction are increasing year by year.
Therefore, as a kind of cardiovascular disease, acute
myocardial infarction is still a kind of disease should
not be ignored and worthy of study.
REFERENCES
A.D. Bond, R. Boese, G.R. Desiraju, On the polymorphism
of aspirin: crystalline aspirin as intergrowths of two
"polymorphic" domains, Angewandte Chemie
(International ed. in English), 46 (2007) 618-622.
E. Boersma, N. Mercado, D. Poldermans, M. Gardien, J.
Vos, M.L. Simoons, Acute myocardial infarction,
Lancet (London, England), 361 (2003) 847-858.
F.L. Kaufman, A.S. Dubansky, Darvon Poisoning with
Delayed Salicylism: A Case Report, Pediatrics, 49
(1972) 610-611.
H.D. White, D.P. Chew, Acute myocardial infarction,
Lancet (London, England), 372 (2008) 570-584.
H.-C. Diener, J. Bogousslavsky, L.M. Brass, C.
Cimminiello, L. Csiba, M. Kaste, D. Leys, J. Matias-
Guiu, H.-J. Rupprecht, Aspirin and clopidogrel
compared with clopidogrel alone after recent
ischaemic stroke or transient ischaemic attack in high-
risk patients (MATCH): randomised, double-blind,
placebo-controlled trial, The Lancet, 364 (2004) 331-
337.
J.-M. Pereillo, M. Maftouh, A. Andrieu, M.-F. Uzabiaga,
O. Fedeli, P. Savi, M. Pascal, J.-M. Herbert, J.-P.
Maffrand, C. Picard, Structure and Stereochemistry of
the Active Metabolite of Clopidogrel, Drug
Metabolism and Disposition, 30 (2002) 1288-1295.
J.L.M.D.M.P.H. Mega, S.L.P. Close, S.D.M.D. Wiviott,
L.P. Shen, R.D.M.D. Hockett, J.T.M.D. Brandt, J.R.P.
Walker, E.M.M.D. Antman, W.M.D.P. Macias,
E.M.D. Braunwald, M.S.M.D.M.P.H. Sabatine,
Cytochrome P-450 Polymorphisms and Response to
Clopidogrel, The New England Journal of Medicine,
360 (2009) 354-362.
J.-P. Collet, J.-S. Hulot, A. Pena, E. Villard, J.-B. Esteve,
J. Silvain, L. Payot, D. Brugier, G. Cayla, F. Beygui,
G. Bensimon, C. Funck-Brentano, G. Montalescot,
Cytochrome P450 2C19 polymorphism in young
patients treated with clopidogrel after myocardial
infarction: a cohort study, Lancet (London, England),
373 (2009) 309-317.
P. Vishweshwar, J.A. McMahon, M. Oliveira, M.L.
Peterson, M.J. Zaworotko, The Predictably Elusive
Form II of Aspirin, Journal of the American Chemical
Society, 127 (2005) 16802-16803.
R.K. Ferguson, A.R. Boutros, Death following self-
poisoning with aspirin, JAMA, 213 (1970) 1186-1188.
T.D. Warner, J.A. Mitchell, Cyclooxygenase-3 (COX-3):
Filling in the Gaps toward a COX Continuum?,
Proceedings of the National Academy of Sciences of
the United States of America, 99 (2002) 13371-13373.
T. Simon, C. Verstuyft, M. Mary-Krause, L. Quteineh, E.
Drouet, N. Méneveau, P.G. Steg, J. Ferrières, N.
Danchin, L. Becquemont, S.T.E. French Registry of
Acute, S.T.E.M.I.I. Non, Genetic determinants of
response to clopidogrel and cardiovascular events, The
New England journal of medicine, 360 (2009) 363-
375.
ICBEB 2022 - The International Conference on Biomedical Engineering and Bioinformatics
578
