
Epilepsy: GABRB3 Gene and Medical Treatment
Zhichao Dai
1,† a
and Sicheng Pan
2,† b
1
Maple Leaf International School Shanghai, 201501, SH, China
2
The University of New Hampshire, 03824, Durham, NH, U.S.A.
†
These authors contributed equally
Keywords: Epilepsy, GABRB3 Gene.
Abstract: Epilepsy is one of the most common central nervous system disorders and chronic diseases on the existing
human. By writing this essay, we summarize and combine the genetic level with the macroscopic view of the
disease. In definition, epilepsy is described as repeating occurrences of sudden excessive or synchronous
discharge in the cerebral cortical neuron that leading to various symptoms, depending on the brain region it
affects. So, epilepsy is classified into 4 types, focal epilepsy, complex focal seizures, generalized epilepsy,
and combined generalized and focal epilepsy. It is worldwide spread, affecting 50 million people, mostly kids,
and elders, and the prevalence was slightly higher in males than females. At the genetic and molecular biology
level, a strong association of GABRB3(Gamma-aminobutyric acid receptor subunit beta-3) gene and GABAA
receptor it encodes for is shown to epilepsy because of the function of the GABAA receptor is inhibiting nerve
impulses, mutation of the GABRB3 gene would psychologically lead to anxiety and restlessness, physically
disorders like epilepsy. Based on looking and summarizing the macroscopic aspects of the disease, brain
activities, and genetic views, we suggest therapies like CRISPR on the GABRB3 gene would likely to provide
treatments for epilepsy in the future.
1 INTRODUCTION
1
Epilepsy is very time-honored and is with the
continuous development of human civilization and
development. The earliest descriptions were in texts
written in 2000 BC in Akkadian and used in
Mesopotamia. Descriptions related to epilepsy also
appeared in the many ancient civilizations, such as
ancient Egyptian, ancient Babylon, and ancient
Greek. In this ancient literature, epilepsy was
generally considered as evil spirits or divine
punishment. This occult interpretation continued to
influence what people thought about epilepsy until
the appearance of Hippocrates. Hippocrates raised the
first formal description of epilepsy as a kind of
disease, and in his classic treatise on the Sacred
Disease, he said that epilepsy was not more sacred
than any other disease, and it had the same properties
as other diseases and some causes of individual
diseases. Complete liberation of epilepsy from
superstition appeared in the 18th and 19th centuries,
although the description that epilepsy is a kind of
a
https://orcid.org/0000-0002-3338-1431
b
https://orcid.org/0000-0002-1645-9161
disease appeared at the Hippocrates times. And the
most important progresses that appeared in the 20th
century included the invention of
electroencephalograph (EEG), the advance in
neurosurgery, the discovery of antiepileptic drugs,
and the delineation of underlying pathophysiological
mechanisms. And because of these progresses, the
myth about epilepsy has been shattered, and social
acceptance has risen to a new level. When doing a
general survey about epilepsy’s history, epilepsy is so
important that attract scientists and doctors from
ancient times to the present constantly explore and try
the solutions of the cure of epilepsy. And even now,
epilepsy researching is continuing and becomes
deeper into the nature of epilepsy. Science seems to
be dominated by genetic research and advances in
computer and information technology in the 21st
century. The future of epilepsy research is
researching the gene that causes epilepsy, including
the Gamma-aminobutyric acid receptor subunit beta-
3 gene (GABRB3 gene). This article would introduce
760
Dai, Z. and Pan, S.
Epilepsy: GABRB3 Gene and Medical Treatment.
DOI: 10.5220/0011294600003443
In Proceedings of the 4th International Conference on Biomedical Engineering and Bioinformatics (ICBEB 2022), pages 760-766
ISBN: 978-989-758-595-1
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

epilepsy’s basic information, epilepsy-related gene
and discuss some new treatment means.
2 INTRODUCTION OF EPILPESY
Epilepsy is a central nervous system disorder that can
affect the brain and cause frequent seizures. Epilepsy
is a very common neurological and chronic disease
but compared with the other similar chronic disease,
the patients of epilepsy are more likely to have some
physical, social, and psychological problems. By
choosing one hundred patients with epilepsy from the
neurological outpatient department from two
hospitals in Baghdad/Iraq and doing the research, the
study showed that most of the patients with epilepsy
were threatened by death (88%) and felt fear from
epilepsy seizure (77%). More than the half of the
sample expressed feeling disappointment after the
attack. Moreover, the study showed that 86% of the
selected sample were severely affected by the social
stigma and 64% of the selected sample thought they
were a heavy burden for their family. This series of
evidence shows that the psychological combat from
epilepsy is very serious and can affect other aspects
of life for patients. The patients of epilepsy are
difficult to have marriage and children because they
are afraid of their children have epilepsy and studies
in many countries and cultures have shown that many
families still oppose their children marrying epilepsy
patients because they believed that the epilepsy
patients were unable to meet their social and
economic needs roles and obligations.
When a seizure happens, repeated occurrences of
sudden excessive or synchronous discharge in
cerebral cortical neurons result in a disruption of
unconsciousness, disturbance of sensation,
movement, and impairment of mental function. It is
different between epilepsy and seizures, while
epilepsy and seizure are often mixed. A seizure is a
single occurrence; however, epilepsy is a
neurological condition characterized by two or more
unprovoked seizures.
2.1 Types of Epilepsy
Epilepsy has four types: focal epilepsy, complex focal
seizures, generalized epilepsy, and combined
generalized and focal epilepsy. These four types of
epilepsy are identified by various brain positions
where sudden excessive or synchronous discharges
are repeated. Generalized epilepsy is the seizures
happening that involve all areas of the patient’s brain;
nevertheless, focal epilepsy can appear to involve just
the specific area of the brain. And the combined
generalized and focal epilepsy is like the suggestion
of the name, which is a form of epilepsy, and patients
have both generalized and focal seizures. It is very
important to identify the types of epilepsy because
one medication may treat one specific type of
epilepsy well but may worsen another type of
epilepsy simultaneously.
2.2 Prevalence of Epilepsy
The prevalence of epilepsy is the proportion of any
population affected by epilepsy at a specific time
worldwide. The estimated proportion of the general
population with active epilepsy at a given time is
between 4 and 10 per one thousand people. And
epilepsy affects around 50 million people in the
world. Moreover, an estimated five million people are
diagnosed with epilepsy each year globally. But it is
worth noticing that the reported incidence of epilepsy
(the rate of new cases in the population) is different
between high-income and low-income economies.
The incidence of epilepsy in high-income economies
is obviously lower than the incidence in low-income
economies. In fact, nearly 80% of people with
epilepsy live in low-and middle-income countries.
However, one study showed that although the
incidence of epilepsy is higher in low- and middle-
income countries, the lifetime prevalence appears to
be roughly the same worldwide. According to a data
review, lifetime epilepsy ranged from 3.2 to 30.1 per
1,000 population in high-income economies, from 4.5
to 18.6 in upper-middle-income economies, from 2.5
to 32.1 in lower-middle-income economies, and from
4.7 to 23.3 in low-income economies.
Besides regional differences in income levels,
epilepsy prevalence is different by gender, which the
prevalence of males with epilepsy is slightly higher
than females with epilepsy. The Rochester epilepsy
study found that the prevalence of epilepsy was
slightly higher in males than females, and the
proportion between males and females is about 6.5 to
6.0 per 1000 persons. The reason that causes this
condition may be the various prevalence of the most
common risk factors in gender and the concealment
of the condition in women for sociocultural reasons
in certain regions.
2.3 The Symptoms of Epilepsy
The symptoms of epilepsy have a great variety and
exist huge differences between them. Overall,
epilepsy symptoms mainly include staring at the
empty space, temporary confusion, uncontrollable
Epilepsy: GABRB3 Gene and Medical Treatment
761

jerking of limbs, losing consciousness and awareness,
and psychically fear, anxiety, or deja vu. However,
patients with different types of epilepsy may have
some of these symptoms. And even if two patients
have the same kind of epilepsy, the symptoms
between them may be totally different. For example,
generalized tonic-clonic seizures are the most well
recognized, also called ‘grand mal seizures in the
past. When these seizures happen, the first symptom
is a sudden loss of consciousness, and then the body
would become stiff, followed by jerking of the
muscles. And often, patients may turn red or blue, bite
their tongue, and lose control of the bladder, but these
symptoms vary with each individual. In addition, the
symptoms of generalized absence seizures are much
milder and briefer than generalized absence seizures,
although they belong to generalized seizures. The
symptoms of generalized absence seizures involve
staring, loss of expression, unresponsiveness, and
stopping activity. And sometimes, the patients with
generalized absence seizures just show eye blinking
or upward eye movements.
2.4 The Risk Factors of Epilepsy
Epilepsy is a complex disease with many causes, and
seizures can be led by caused by anything that
disrupts the normal electrical patterns of the brain.
Epilepsy has no identifiable cause in about half the
people with the condition. In the other half, the
condition may be traced to various factors, including
genetic influence, head trauma, brain conditions,
infectious diseases, prenatal injury, and
developmental disorders. First, epilepsy is considered
a high genetic disease, and under many conditions,
epilepsy can be heritable. For example, in idiopathic
generalized epilepsy, the first-degree relatives of
epilepsy patients have an 8-12% risk of developing
epilepsy, which is much higher than the risk in the
general genetic component. Then head trauma is
related to epilepsy, and the recurrent seizure disorder
because of injury to the brain following head trauma
is called Posttraumatic epilepsy (PTE). Studies
showed that traumatic brain injury makes up about
10-20 % of symptomatic epilepsy in the general
population and 5% of all epilepsy. Third, infectious
and infestations are one of the most common risk
causes for seizures and acquired epilepsy and maybe
the most common preventable risk factor for epilepsy
worldwide, especially in resource-poor countries.
Many types of infectious diseases can develop
seizures, ranging from toxoplasma in the newborn,
early childhood infection with human herpesvirus
(HHV)-6 to Creutzfeldt-Jakob disease (CJD) in the
elderly. And seizures maybe just one symptom in
some infectious diseases such as neurocysticercosis
(NCC). Then, prenatal injury can also result in
epilepsy, which is brain damage before babies’ birth
that could be caused by several factors, such as poor
nutrition or oxygen deficiencies. Finally, sometimes
epilepsy can have linkage with developmental
disorders, such as autism and neurofibromatosis.
2.5 The Brain Activity of Epilepsy
The brain activity of epilepsy is the key to a cure for
epilepsy. By researching the brain activity of
epilepsy, scientists can know better the mechanism of
action of epilepsy, influencing factors, and so on,
which provides some new ideas to find the cure
methods for epilepsy. Because the brain activity of
epilepsy is hard to observe and some moral and
ethical barriers and so on, the research of the brain
activity of epilepsy is not very rich and impeccable. It
is hard to observe the brain activity directly, and
scientists have to use some roundabout methods to
research the brain activity of epilepsy, for example,
using the method that compares with the healthy
control group. The main method to detect brain
activity is using a series of scientific instruments,
such as electroencephalography (EEG), magnetic
resonance imaging (MRI), High-density
electroencephalography. EEG is used to record the
brain's electrical activity, which is also the most
common and basic method of detecting epileptic
activity. But although EEG has high temporal
resolution and sensitivity, it is less spatial resolution
and is not sensitive to an activity deep in the brain.
Moreover, EEG can only detect abnormal signals
when the seizure happens, so EEG also has some
imperfections. MRI is often used cooperatively with
EEG to make the detection method more impeccable
because of its better spatial resolution. To be sum,
these are only short-term brain activities.
2.5.1 Short-term Brain Activity
The brain activity of epilepsy researching can be
divided into short-term changes and long-term
changes. The most obvious brain change for short-
term brain activity is the repeated occurrences of
sudden excessive or synchronous discharge in the
cerebral cortical neuron. These discharges can be
detected by EEG and be used to help doctors make a
diagnosis of epilepsy. The EEG of epilepsy which is
different from normal EEG, is called epileptiform
discharge, and it occurs in up to 98% of patients with
epilepsy depending on age and epileptogenicity. The
ICBEB 2022 - The International Conference on Biomedical Engineering and Bioinformatics
762

patterns of the epileptiform discharges are considered
to have the following types: spikes, sharp waves,
benign epileptiform discharges of childhood, spike-
wave complexes, slow spike-wave complexes, 3-Hz
spike-wave complexes, polypiles, hypsarrhythmia,
seizure pattern, and status pattern. Although
epileptiform discharge has many patterns, the
epileptiform discharge has no objective definition,
and even experienced electroencephalographers
sometimes feel confused about the diagnosis of
epileptiform.
2.5.2 Long-Term Brain Activity
For long-term brain changes of epilepsy, epilepsy can
alter patients’ neuromagnetic activities and brain
network in the high-frequency ranges. These
alterations become more pathological as the duration
of epilepsy grows longer. According to new research
led by the UCL Institute of Neurology and the Keck
School of Medicine of USC, the team found reduced
grey matter thickness in parts of the brains’ outer
layer and reduced volume in subcortical brain regions
in all epilepsy groups when compared to the control
group. And from a study of children’s epilepsy,
seizures alter brain functions by over activating,
interrupting, or destroying vital networks of brain
activity. It is clear that epilepsy has profound effects
on the developing child’s brain. About half of
children with epilepsy experience learning
difficulties, especially those involving problems with
attention and memory.
3 EPILEPSY AND THE GAMMA-
AMINOBUTYRIC ACID
RECEPTOR SUBUNIT BETA-3
GENE (GABRB3 GENE)
In the molecular neurobiology domain, well-known
disorders like autism spectrum disorder (ASD),
bipolar disorder, and schizophrenia disorder are
proved to have a strong relationship with mutation of
genes of neurological structures like some
neurotransmitters and synaptic receptors that
influence not only mental aspects but also the ability
to coordinate and movements. In the case of epilepsy,
the most related gene is the Gamma-aminobutyric
acid receptor subunit beta-3 gene.
3.1 The Gamma-Aminobutyric Acid
Receptor Subunit Beta-3 Gene and
the GABAA Receptor
Research and studies have shown that the mutation of
the Gamma-aminobutyric acid receptor subunit beta-
3 gene and the protein it codes for have a significant
association with many neurodevelopmental disorders
other than Epilepsy, like Angelman syndrome and
autism. By analysing this particular gene and protein,
more treatments and therapies could be found to aim
at those common disorders that this gene involved in.
Going back to the mid-1950s, researchers and
experimenters had made dozens of efforts on gamma-
aminobutyric acid in both humans and animals’
brains, and how some available drugs like
benzodiazepines and barbiturates (function as
enhancing the currents of GABAA receptor) which
could affect GABAA receptor that it is one of the
most common prolific targets for therapeutic.
3.2 The GABRB3 Gene
The belief that the GABRB3 gene is associate with
epilepsy and childhood absence epilepsy (CAE)
originated from the team of Lydia Urak, who
analysed this gene’s single nucleotide
polymorphisms (SNPs) in particular exons. They
tested 45 patients of CAE in the Medical University
of Vienna, and the results showed that the strong
association of CAE with 13 single nucleotide
polymorphisms in the GABRB3 gene, from exon 1a
promoter to the beginning of intron 3 among 45
subjects. The GABRB3 gene is located at
chromosome 15, region q12 of the human genome. It
has 10 exons in its coding region, and since the
alternative splicing, the GABRB3 gene could code
for various other protein isoforms that are subunits of
the GABAA receptor.
GABRB3 gene is frequently expressed in the
human brain during the proliferation and
differentiation of human embryonic developments. In
contrast, it is not expressed in the adult brain
extensively except the hippocampus.
Epilepsy: GABRB3 Gene and Medical Treatment
763
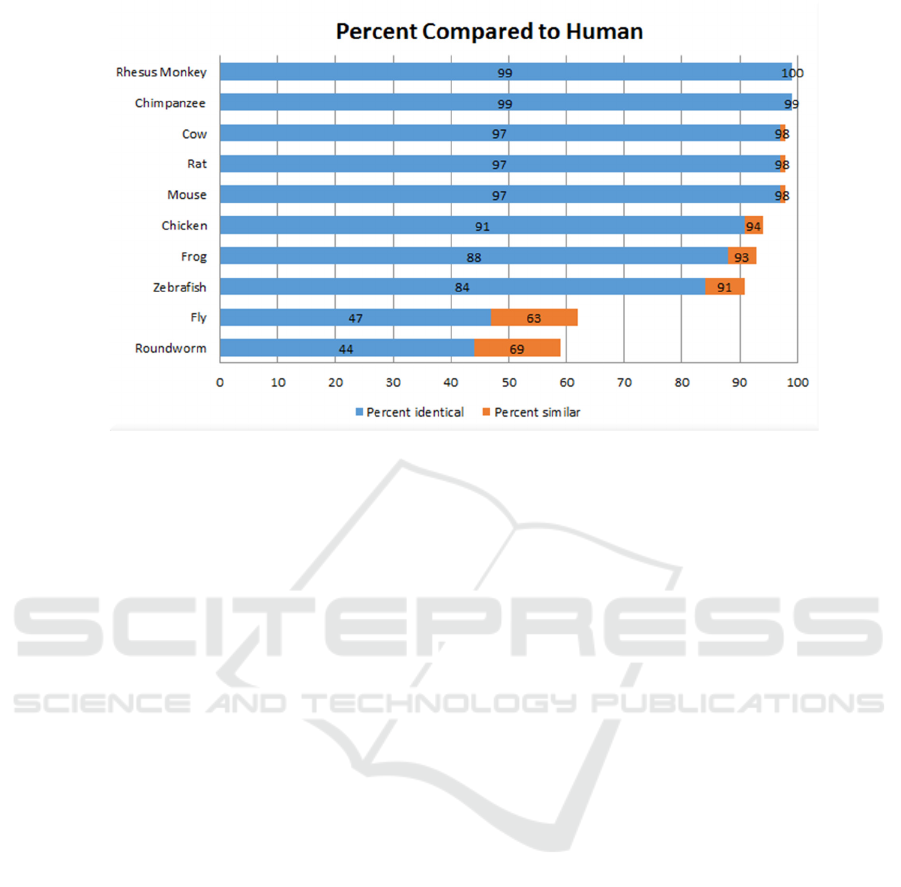
Figure 1: Conserveness of GABRB3 protein across different species and the sharing similarities.
3.3 The GABRB3 Protein
Studies have shown that the GABRB3 protein is
conserved among various species. Most other
mammals and vertebrates’ gene models are similar to
humans, k, some even have identically matched over
90%, especially the Chimpanzee and Rhesus
monkeys. This illustrates the importance of this gene
that the protein it encodes is necessary for the
neuronal growth of the Craniata species and animals
in lower classes. There are over 10 types of subunits
combined to form a chloride channel (for example,
GABAA receptor), and the GABRB3 protein is one
of those, which will be discussed in detail in the next
chapter.
3.4 The GABA and the GABAA
Receptor
The Gamma (γ) -aminobutyric acid (GABA) is one of
the most important inhibitory neurotransmitters
involves in the central nervous system (CNS)
development. As its reducing function acts on the
inhibiting excitabilities of neurons, it would
hyperpolarize the neurons at the resting potential of
the action potential by binding to GABAA receptor
or GABAAR and GABAB receptor or GABABR.
The GABA controls all excitabilities areas in the
human brain with another neurotransmitter. To keep
a balance in the brain, those excitabilities are
regulated by both the GABAergic activities and
glutamatergic neurons, which produce the most
common and critical excitatory neurotransmitters —
glutamate that stimulates action potentials. In
opposite, the inhibitory neurotransmitters GABA in
GABAergic activities inhibits action potentials.
When two of these neurotransmitters could not
function properly depending on situations, symptoms
like anxiety, restlessness, insomnia, and even
disorders like schizophrenia and Parkinson's disease
would occur when reducing the GABAergic
activities. In addition, sedation, amnesia, and ataxia
will appear when the GABAergic activities outweigh
the glutamatergic activities. And the neurotransmitter
GABA is manufactured by GABAergic neurons,
which are neurons that use and produce GABA as
their neurotransmitter that is commonly distributed in
the CNS but not common outside the brain and in the
spinal cord.
The GABA receptor that is significant to epilepsy
is code by GABRB3, the GABAA receptor. It is
wildly distributed in the human brain that it could be
found in 20% to 50% of all the brain synapses. The
GABAAR and GABA are most concentrated in the
human limbic system that involves human emotions
and memories, especially when one is under a strong
feeling or challenges and traumas. And the GABAA
receptor is only one of the receptors that could be
activated by GABA, an ionotropic receptor and
ligand-gated ion channel. By allowing the permeation
of chloride ions (Cl−) in or out of the membrane, its
function is to maintain or mediate the synaptic
membrane potential and inhibit action potentials.
ICBEB 2022 - The International Conference on Biomedical Engineering and Bioinformatics
764
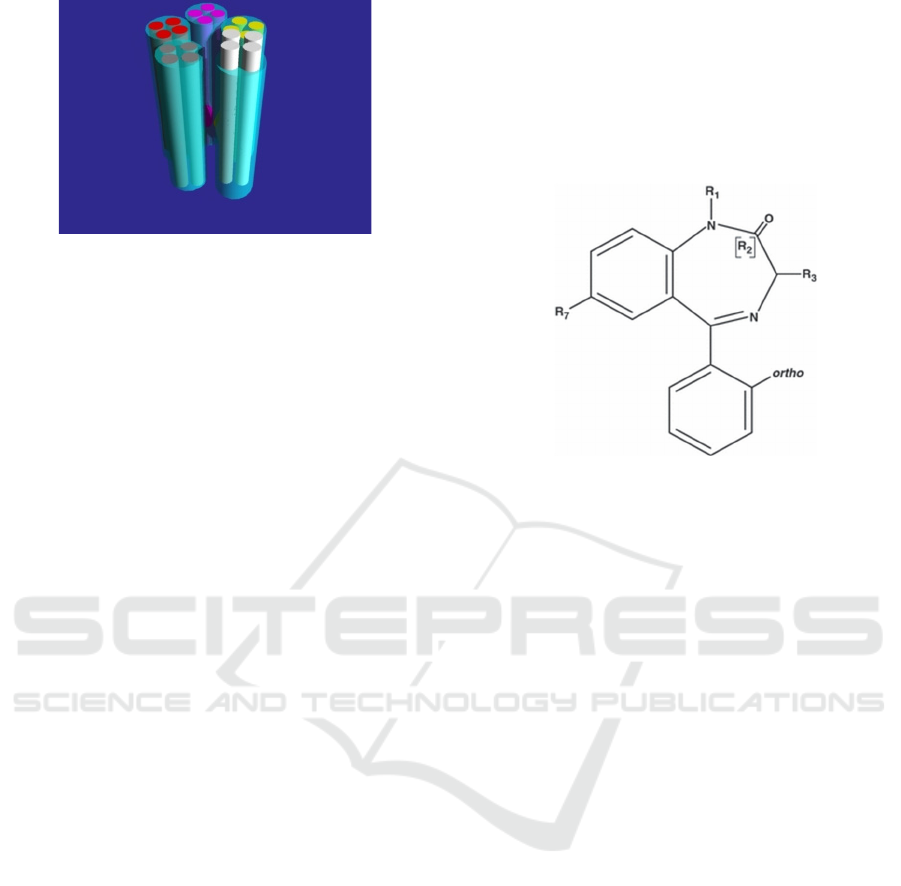
Figure 2: Structure of GABAA receptor, within 5 subunits
composed a channel in the middle.
The structure of the GABAA receptor is quite
normal, just like most other ligand-gated receptors, it
is formed by five subunit proteins, that each of which
is about 50,000 Daltons in size, and every last one of
these amino acid strings goes into and out the cell
membrane 4 times, leaves an N-terminal at the
extracellular space, which is the end of the
polypeptide that, it would function as mediating the
channel’s interactions. And in the middle of those
amino acids, there is a large area of looping inside,
with four sites where phosphorylation occurs. Those
subunits that composed to this receptor have been
classed into α1–α6, β1–β3, γ1–γ3, δ, ε, π, θ, and ρ1–
ρ3. It seems alpha and beta are the key components of
GABAA receptors since most of them are arranged
by two alpha and beta subunits in the limited 5
maximums.
When GABA binds to the GABAA receptor, the
ion pore in the middle will open, which facilitates the
influx or efflux of chloride ions (Cl-), depending on
the concentration difference of Cl- outside and inside
the cell that regulates by the potassium chloride
(KCC2) and sodium-potassium chloride (NKCC1)
co‐transporters.
3.5 Medical Treatment of Epilepsy:
Benzodiazepines
Benzodiazepines (BZDs), as mentioned, are one of
the most significant medical agents of epilepsy since
the 1960s. They are targeted on the GABAA
receptors, that they have had a strong preference
towards status epilepticus and seizures. Besides,
BZDs have also been used in febrile or repetitive
seizures and alcohol withdrawal seizures. They
became the first choice when those symptoms came
since they have high efficacy, rapid onset, and less
toxicity on functions like sedation, anxiety-reducing,
and muscle relaxation. Each type of BZD shows
different pharmacologic effects according to
particular symptoms, and among all of these 35 kinds
of BZDs, there are some used in epilepsy. When
BZDs bind to the GABAA receptor, they are not
substituting the GABA but acting as an enhancing
agent to provide more chances of the channel opening
to allow more Cl- get in or out to increase or decrease
the current. The BZDs are sharing a structure of a
benzene ring and seven-membered diazepine ring
fusion.
Figure 3: General chemical structure of 1,4-
benzodiazepines
4 CONCLUSIONS
This dissertation resulted from an investigation into
the macroscopic level, molecular biology, and genetic
level of epilepsy. It concentrated on the symptoms
and brain activity of epilepsy, mutation of GABAA
receptor, and its gene. As an overview, the current
state of knowledge we had summarized about
epilepsy shows a strong association it has with the
GABRB3 gene. Still, since the limitation of more
recent data of how epilepsy is prevalent beyond all
ages, genders, and regions and the genetic experiment
of GABRB3 gene, further research needs to be
conducted on those aspects.
REFERENCES
Atack, John R et al. “Rat pharmacokinetics and
pharmacodynamics of a sustained release formulation
of the GABAA alpha5-selective compound L-
655,708.” Drug metabolism and disposition: the
biological fate of chemicals vol. 34,5 (2006): 887-93.
doi:10.1124/dmd.105.006973
Beghi E. The Epidemiology of Epilepsy. (2020)
https://www.karger.com/Article/Fulltext/503831
BELL G, NELIGAN A, SANDER J,. An unknown
quantity-The worldwide prevalence of epilepsy[J].
Epilepsia, 2014, 55(7): 958-962.
Epilepsy: GABRB3 Gene and Medical Treatment
765

Blandini, F et al. “Glutamate and Parkinson's disease.”
Molecular neurobiology vol. 12,1 (1996): 73-94.
doi:10.1007/BF02740748
CEREGHINO J,. The major advances in epilepsy in the
20th century and what we can expect (hope for) in the
future[J]. Epilepsia, 2009, 50(3): 351-357.
Chavezgen. “Asperger's Syndrome and the GABRB 3
Gene.” chavezgen564s14.weebly.com/homology.html.
DUNN D, KRONENBERGER W,. Childhood Epilepsy,
Attention Problems, and ADHD: Review and Practical
Considerations[J]. Seminars in Pediatric Neurology,
2005, 12(4): 222-228.
Egerton, Alice, et al. "Glutamate in schizophrenia:
neurodevelopmental perspectives and drug
development." Schizophrenia Research (2020).
Epilepsy - Symptoms and causes[EB/OL]. Mayo Clinic,
2021. (2021) [2021 -07 -19].
https://www.mayoclinic.org/diseases-
conditions/epilepsy/symptoms-causes/syc-20350093.
Epilepsy Linked to Brain Volume and Thickness
Differences[EB/OL]. Neuroscience News, 2021.
(2021) [2021 -08 -05].
https://neurosciencenews.com/epilepsy-brain-
thickness-volume-8348/.
Epilepsy[EB/OL]. Healthdirect.gov.au, 2021. (2021) [2021
-07 -19]. https://www.healthdirect.gov.au/epilepsy.
Feldman RS, Meyer JS, Quenzer LF. Principles of
neuropsychopharmacology. Sunderland, MA: Sinauer
Associates, Inc., 1997; 673–729.
https://www.healthline.com/health/epilepsy/types-of-
epilepsy#types-of-epilepsy.
INTISAR K, FAKHRIA M,. Impact of epilepsy on patient's
physical and psychosocial functioning: iraqi
study[EB/OL]. Hsj.gr, 2021. (2021) [2021 -07 -19].
https://www.hsj.gr/medicine/impact-of-epilepsy-on-
patients-physical-and-psychosocial-functioning-iraqi-
study.php?aid=3186.
Macdonald, R L, and R W Olsen. “GABAA receptor
channels.” Annual review of neuroscience vol. 17
(1994): 569-602.
doi:10.1146/annurev.ne.17.030194.003033
Macdonald, Robert L., and M. A. Rogawski. "Epilepsy: a
comprehensive textbook." (2008): 1433-1445.
Macdonald, Robert L., and Richard W. Olsen. "GABAA
receptor channels." Annual review of neuroscience 17.1
(1994): 569-602.
MAGIORKINIS E, DIAMANTIS A, SIDIROPOULOU K
et al.. Highights in the History of Epilepsy: The Last
200 Years[J]. Epilepsy Research and Treatment, 2014,
2014: 1-13.
MAGIORKINIS E, SIDIROPOULOU K, DIAMANTIS
A,. Hallmarks in the history of epilepsy: Epilepsy in
antiquity[J]. Epilepsy & Behavior, 2010, 17(1): 103-
108.
NAGHAVI M,. Global, regional, and national burden of
suicide mortality 1990 to 2016: systematic analysis for
the Global Burden of Disease Study 2016[J]. BMJ,
2019: l94.
NOACHTAR S, RÉMI J,. The role of EEG in epilepsy: A
critical review[J]. Epilepsy & Behavior, 2009, 15(1):
22-33.
NUNEZ K,. Types of Epilepsy and Seizure Disorders,
Causes and Symptoms [EB/OL]. Healthline, 2021.
(2021) [2021 -07 -12].
Nutt, David J., and Andrea L. Malizia. "New insights into
the role of the GABAA–benzodiazepine receptor in
psychiatric disorder." The British Journal of Psychiatry
179.5 (2001): 390-396.
Papandreou, Apostolos et al. “GABRB3 mutations: a new
and emerging cause of early infantile epileptic
encephalopathy.” Developmental medicine and child
neurology vol. 58,4 (2016): 416-20.
doi:10.1111/dmcn.12976
PITKÄNEN A, BOLKVADZE T,. Head trauma and
epilepsy[J]. Epilepsia, 2010, 51: 31-31.
PODURI A, LOWENSTEIN D,. Epilepsy genetics—past,
present, and future[J]. Current Opinion in Genetics &
Development, 2011, 21(3): 325-332.
Riss, J1, et al. "Benzodiazepines in epilepsy: pharmacology
and pharmacokinetics." Acta neurologica scandinavica
118.2 (2008): 69-86.
ROBERTS, E, and S FRANKEL. “gamma-Aminobutyric
acid in brain: its formation from glutamic acid.” The
Journal of biological chemistry vol. 187,1 (1950): 55-
63.
Shader RI, Greenblatt DJ. Benzodiazepines: some aspects
of their clinical pharmacology. Ciba Found Symp 1979;
74:141–55.
Tanaka, Miyabi, et al. “GABRB3, Epilepsy, and
Neurodevelopment.” Jasper's Basic Mechanisms of the
Epilepsies, edited by Jeffrey L Noebels et. al., 4th ed.,
National Center for Biotechnology Information (US),
2012.
TEDRUS G, FONSECA L, PEREIRA R,. Marital status
of patients with epilepsy: Factors and quality of life[J].
Seizure, 2015, 27: 66-70.
Urak, Lydia, et al. "A GABRB3 promoter haplotype
associated with childhood absence epilepsy impairs
transcriptional activity." Human molecular genetics
15.16 (2006): 2533-2541.
VEZZANI A,. Epilepsy and Inflammation in the Brain:
Overview and Pathophysiology[J]. Epilepsy Currents,
2014, 14(2_suppl): 3-7.
ZENG H, PIZARRO R, NAIR V et al.,. Alterations in
regional homogeneity of resting-state brain activity in
mesial temporal lobe epilepsy[J]. Epilepsia, 2013,
54(4): 658-666.
Zimmerberg, Betty, et al. “III. Neurotransmitter
Postsynaptic Receptors” Williams College
Neuroscience (1998): 3.2-3.5 <
https://web.williams.edu/imput/IIIA5.html >.
ICBEB 2022 - The International Conference on Biomedical Engineering and Bioinformatics
766
