
A Medical Information System for Personalized Rehabilitation after
Ankle Inversion Trauma
Jonathan Neugebauer
1 a
, Rosemary Dubbeldam
2 b
, My Linh Pham
1
, Lokman Beser
1
,
Luka Gerlach
1
, Yu Yuan Lee
2
and Herbert Kuchen
1 c
1
Department for Information Systems, University of M
¨
unster, M
¨
unster, Germany
2
Institute of Sport and Exercise Sciences, University of M
¨
unster, M
¨
unster, Germany
Keywords:
Medical Informatics, Clinical Decision Support System, Mobile App, Domain Specific Language,
Model-driven Software Development.
Abstract:
We have developed FEAL, a mobile app and a corresponding server component supporting personalized re-
habilitation after an ankle inversion trauma. In order to enable the maintenance of the essential parts of the
overall system by health professionals, an easy to understand domain specific language (DSL) has been de-
signed enabling them to adapt the questionnaires which are essential parts of the app. For the same reason, the
included medical knowledge is not hard coded in a programming language but provided by rules of a business
rules management system. A DSL specification is automatically transformed by a correspondingly developed
generator to platform-independent React Native code such that the resulting app can be used on the relevant
platforms iOS and Android.
1 INTRODUCTION
Particularly physically active people frequently suf-
fer from ankle sprains. Up to 40 % of these cases can
eventually escalate to chronic ankle instability (Hertel
and Corbett, 2019). In order to prevent this, patients
need to execute appropriate exercises which should
be adapted to their current state and patients need to
be informed about their injury and the expected reha-
bilitation process. Thus, we have developed FEAL,
a mobile app suggesting and explaining personalized
exercises to the patient and providing injury and re-
habilitation related information. The required med-
ical knowledge cannot be stored on the mobile de-
vice running the app. It rather has to be provided by
a server to which the app connects if needed. The
medical knowledge is on the state of the art. Nev-
ertheless, it has to be updated, if new insights have
been found. This maintenance should ideally be per-
formed by a health professional rather than by a soft-
ware developer. Thus, the medical knowledge has to
be provided in a form which can be maintained by
health professionals. Hence, it cannot be expressed
a
https://orcid.org/0000-0001-5865-7118
b
https://orcid.org/0000-0001-7471-9737
c
https://orcid.org/0000-0002-6057-3551
in a classic programming language. Instead, we use
when-then rules of a business rules management sys-
tem (BRMS) (Boyer and Mili, 2011). In our case,
we use the BRMS Drools
1
. In addition to the rules,
the server also stores data about the rehabilitation of
the patients, which can later on be used for scientific
studies.
The mobile app needs to ask patients about the
current state of their ankle impairments and their ex-
periences when performing the suggested exercises.
Based on the answers, new exercises are suggested
after involving the rules engine on the server side. A
large part of the app is a questionnaire. Again, this
questionnaire is also subject to changes which should
ideally be performed by a health professional rather
than by a software developer. Thus, a questionnaire
should be expressed on a high level of abstraction and
in a way health professionals can understand. There-
fore, we have developed a domain specific language
(DSL) (Voelter et al., 2013) which allows to design
such a questionnaire. Since both, the medical knowl-
edge and the questionnaire, are not hard coded in a
programming language but provided in a form where
they can easily be adapted, our approach is not lim-
ited to the rehabilitation of ankle inversion trauma but
1
https://www.drools.org
Neugebauer, J., Dubbeldam, R., Pham, M., Beser, L., Gerlach, L., Lee, Y. and Kuchen, H.
A Medical Information System for Personalized Rehabilitation after Ankle Inversion Trauma.
DOI: 10.5220/0011295800003266
In Proceedings of the 17th International Conference on Software Technologies (ICSOFT 2022), pages 319-330
ISBN: 978-989-758-588-3; ISSN: 2184-2833
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
319

it can also be used in other medical areas with a sim-
ilar combination of app, questionnaires, and medical
knowledge expressed by rules.
Finally, the app needs to be platform-independent,
since patients are using different mobile devices based
on the operating systems iOS and Android. Com-
mon techniques for reaching such independence in-
clude the hybrid, interpreted, and cross-compiled ap-
proach (Biørn-Hansen et al., 2018). In the hybrid ap-
proach, apps are implemented using web technologies
and displayed within a native web component. By
relying on web technologies, the interface can only
imitate the look of native interface elements. The in-
terpreted approach, on the other hand, allows for us-
ing native interface components which are rendered
based on, e.g., JavaScript code interpreted during run-
time. In contrast, the cross-compiled approach does
not perform such transformations to native code dur-
ing run-time but during compile-time.
We have deliberately chosen React Native
2
which
follows the interpreted approach. Thus, with the same
code base, apps for iOS and Android can be devel-
oped. Following the model-driven software develop-
ment approach (Stahl and V
¨
olter, 2006), DSL specifi-
cations are automatically transformed into React Na-
tive code. This is done by a corresponding generator
which we have developed, too.
In our work, we followed the design science re-
search methodology (Peffers et al., 2007). From a
software engineering point of view, the main contri-
butions of this application paper are:
• development of an architecture for a mobile app
and a corresponding server supporting the reha-
bilitation after an ankle inversion trauma,
• design of a DSL for expressing corresponding
questionnaires on a high level of abstraction,
• development of a generator transforming DSL
specifications into React Native code,
• development of a set of rules expressing the cor-
responding medical knowledge.
The rest of this paper is organized as follows. In
the next section, we will provide medical background
for our app FEAL. Section 3 presents the overall ar-
chitecture of our approach. More details about the
development will be given in Section 4. In Section 5,
we will discuss our approach. Related work is men-
tioned in Section 6. Finally in Section 7, we conclude
and point out future work.
2
https://reactnative.dev
2 MEDICAL BACKGROUND
An ankle inversion trauma occurs when the ankle
joints are twisted into a too extreme inverted posi-
tion, frequently combined with extension of the ankle
joints. As a result, the ankle ligaments can be par-
tially damaged or completely torn, depending on the
severity of the trauma. Below, first the injury preva-
lence and participation consequences are presented.
Then, measures which influence injury rehabilitation
are briefly discussed.
2.1 Prevalence and Consequences
Ankle sprains are common, and the potential conse-
quences are unfortunately often downplayed. Most
patients and even health professionals consider an an-
kle sprain as a minor injury, much less severe than
for example a strained or torn cruciate ligament of the
knee. Such opinions are not justified if one considers
the 35% to 70% recurrence rate. Even 6-12 months
after the injury, 50% of the patients are still suffering
from minor to major chronic impairments, and about
10% of them cannot return to sports or work (Her-
tel and Corbett, 2019; van Putte-Katier et al., 2015).
Hence, the consequences of this underrated ankle in-
jury are severe. Medical practitioners have very lim-
ited time to provide information about the injury and
rehabilitation process and, in general, only prescribe
an ankle brace for the more severe cases and advise
rest for the less severe cases. Physical therapy is
rarely prescribed even though studies report a 60%
reduced risk of re-injury after balance training (Eils
and Rosenbaum, 2001). About half of the patients
may seek help in the form of information in the avail-
able media or online. However, such information is
usually quite general, mostly not scientifically based,
and certainly not adapted to the individual suffering
from the ankle injury. Bystanders, such as trainers or
coaches, are generally not educated to support injury
rehabilitation.
2.2 Rehabilitation Process
Deviations from the normal regeneration of balance,
gait and jumping or landing abilities predict chroni-
fication of the ankle injury (Doherty et al., 2016).
Hence, it is important to restore impaired functions.
Several typical impairments can be addressed by the
patient. For example, static stretching has a posi-
tive effect on the ankle dorsiflexion range of motion
(Terada et al., 2013); Balance training and muscle
strengthening yield improves balance and reduces re-
current injury risk (Eils and Rosenbaum, 2001). Val-
ICSOFT 2022 - 17th International Conference on Software Technologies
320
Questionnaires
Assessments
Rule
Evaluation
Exercises Feedback
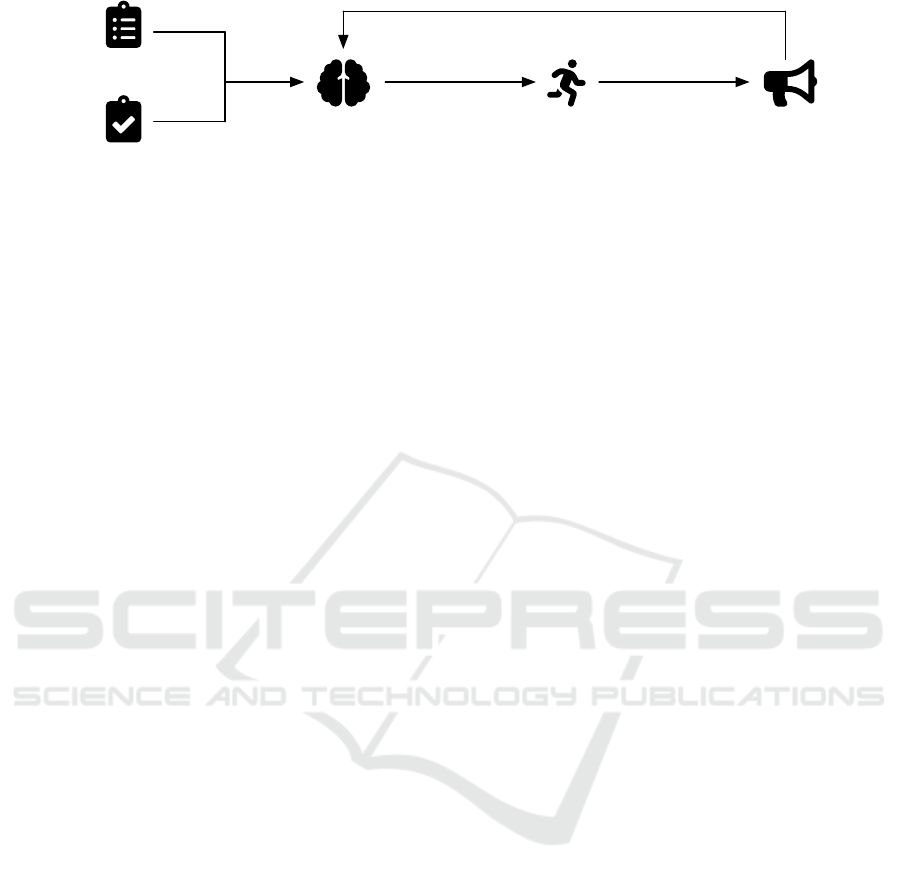
Figure 1: Main phases of the rehabilitation process supported by the medical information system.
idated tools which have been related to the rehabil-
itation process include the Foot and Ankle Ability
Measure (FAAM), the Cumberland Ankle Instabil-
ity Tool (CAIT) and Fear-Avoidance-Beliefs Ques-
tionnaire (FABQ) (Hertel and Corbett, 2019; Hous-
ton et al., 2015). Such tools and simple assessments
of structural function and activities should be used to
monitor the patient’s progress. Thus, our idea was
to develop a mobile app and a corresponding server
backend in order to support the rehabilitation of pa-
tients by suggesting exercises which are tailored to
the current state of the patient.
3 SYSTEM DESIGN
In this section, the medical information system sup-
porting personalized rehabilitation after an ankle in-
version trauma is designed. First, the requirements
are discussed in Subsection 3.1. Based on this, Sub-
section 3.2 outlines the software architecture.
3.1 Requirements Analysis
There are two main stakeholders involved in the re-
habilitation process: the patient and the health pro-
fessional. Throughout the rehabilitation process, the
patient continuously provides information concerning
his or her health condition through the system. The
health professionals, on the other hand, use this infor-
mation to monitor and evaluate the user’s impairments
in structural function and activities and adapt the reha-
bilitation accordingly. Some parts of this adaption can
be done based on rules expressing the current medical
knowledge. Such rules are intended to be evaluated
automatically using a rules engine.
In Figure 1, the main phases of the rehabilitation
process, which the system is intended to support, are
illustrated. The following paragraphs elaborate on
each of these phases.
Questionnaires. At first, the patient answers different
questionnaires, e.g., concerning types of physical ac-
tivity the patient has done lately or the pain sensation
in certain situations. Some questionnaires are more
general while others specifically target ankle impair-
ments. Examples for such questionnaires are the
international physical activity questionnaire (IPAQ)
(Craig et al., 2003), the pain self-efficacy question-
naire (PSEQ) (Nicholas, 2007), or the CAIT (Hiller
et al., 2006) mentioned previously. Some question-
naires allow calculating scores from the given an-
swers which are used by the health professionals to
monitor and adapt the rehabilitation process.
Assessments. In addition to questionnaires, a prior
assessment based on exercises or tests performed by
the patient is required. One example is the weight-
bearing lunge test (WBLT) (Bennell et al., 1998) as-
sessing the mobility of the ankle. After doing the as-
sessment, the patient is asked to answer some ques-
tions. For example, a question could ask for sensation
of pain during the assessment or whether it was too
difficult to perform. Furthermore, the patient could
be asked to do a measurement (e.g., distance or time)
indicating how well the patient was able to perform
an exercise or a test.
Rule Evaluation. Based on information collected
through the questionnaires and assessments, rules ex-
pressing the current medical knowledge are evaluated
to determine appropriate exercises the patient should
do as a further training. These exercises are organized
in exercise groups. An exercise group is a collection
of exercises with different difficulty levels regarding
a specific biomechanical aspect (e.g., balance or fore-
foot stance). The rules are used to determine the start-
ing point within an exercise group, i.e., the exercise
with the appropriate difficulty level. Depending on
the assessment, certain exercise groups might be ir-
relevant and, thus, are not recommended for the pa-
tient (e.g., because the patient is able to do the most
difficulty exercise variant without any problems). On
the other hand, an exercise group might not be recom-
mended if a required questionnaire or assessment was
not done yet.
After the starting points within the relevant exercise
groups have been determined, the exercises are prior-
itized. This prioritization is done based on a list of
exercises which are ordered from most easy and most
vital exercise to most difficult exercise or least vital
for daily life activities. For instance, the prioritization
A Medical Information System for Personalized Rehabilitation after Ankle Inversion Trauma
321

lists starts with two limb weight-bearing and ankle
mobilization exercises and the list ends with single-
leg jumps and running exercises. A collection of the
three exercises with the highest priorities is then given
to the patient as homework. In our use case, the pri-
orities of the exercises are fixed and do not depend
on the patient’s input. Instead, the priorities are only
used to rank the exercises that have been determined
by the rules.
Exercises. At this stage, the patient performs the
suggested personalized exercises from the homework
collection daily.
Feedback. After each exercise, the patient evaluates
whether the exercise was “too easy”, “too difficult”,
or “exactly right”. This feedback is used as an addi-
tional input for the rule evaluation. Depending on the
patient’s answers the exercises are adapted and a new
collection of three exercises is assembled for the next
day. If the performed exercise was too easy, a more
difficult variant is recommended next (analogously if
the exercise was too difficult). If the exercise’s diffi-
culty was exactly right, it stays in the homework col-
lection. Depending on the patient’s progress, an exer-
cise group may be removed from the homework col-
lection given the order of the exercises on the exercise
prioritization list.
In addition to the daily feedback on the exercises, the
patient is asked regularly to repeat specific question-
naires and assessments throughout the training phase
to allow for a continuous monitoring of the rehabili-
tation progress.
Based on this description of the rehabilitation pro-
cess several requirements can be identified. They can
be classified according to which user group they con-
cern.
Patients. First, patients should be able to fill out
questionnaires and do assessments using a mobile
app. Additionally, the mobile app should display
the homework collection and provide the means to
give feedback after having done a homework exercise.
Lastly, the app should present a collection of useful
information to the patient (e.g., general information
on the ankle inversion trauma, advice, or support con-
tacts).
Health Professionals. First, health professionals
require a dashboard to monitor the rehabilitation
progress of their patients. For this purpose, plots pro-
viding a basic analysis of the scores calculated for the
answered questionnaires should be presented. To fa-
cilitate a more detailed statistical analysis, the infor-
mation collected through questionnaires and assess-
ments and with the feedback on the exercises should
be saved in a database. Personalized and appropriate
exercises should be determined automatically based
on user input from the questionnaires and assessment
and on the rules specified by the health professionals.
Lastly, health professionals should be able to adapt
the questionnaires.
There are different question types which the sys-
tem needs to handle. Firstly, single-choice as well as
multiple-choice questions should be supported. Ad-
ditionally, open-ended questions are required. Lastly,
for the purposes of our use case it should be possi-
ble that patients can answer certain questions using
a visual analogue scale (VAS) (Hayes and Patterson,
1921). Here, the patient can choose an appropriate
value for a rating scale between two opposing cate-
gories (e.g., “not at all confident” vs. “completely
confident”). An exemplary question from the previ-
ously mentioned PSEQ involving a VAS is depicted
in Figure 3.
3.2 Software Architecture
Based on the requirements analysis conducted in the
previous subsection, this subsection introduces a suit-
able software architecture. In Figure 2, several core
components are illustrated. On the one hand, there
are parts colored in gray involved in code generation
prior to running the app, while the components col-
ored in black are needed at runtime.
There are two components providing a user inter-
face (UI) for the two main stakeholders: the mobile
app and the dashboard. Both receive data from and
send data to the backend through its application pro-
gramming interface (API). Furthermore, the backend
uses a database for persistent storage of information.
We chose MongoDB
3
due to the flexibility such a
document-oriented database offers for the schema de-
sign. The rule evaluation is done by a separate com-
ponent representing the rules engine. Also this com-
ponent features an API enabling the communication
to the backend. The rules are saved in specific rule
files which are loaded into the rules engine upon ap-
plication start. This way, the rule logic can be adapted
by health professionals without the need of touching
the program code of the rules engine. Drools offers
a DSL called drools rule language (DRL) for the pur-
pose of specifying rules. In addition to using DRL for
defining rules, we implemented a DSL named QuApp
allowing to describe questionnaires and mobile apps
within models. Such models can be fed into a code
generator to generate artifacts corresponding to the
models.
While the app model is transformed to JavaScript
code for React Native, a questionnaire model results
in a JavaScript Object Notation (JSON) document that
3
https://www.mongodb.com
ICSOFT 2022 - 17th International Conference on Software Technologies
322

App Model
Rules Engine
Database
Dashboard
Mobile App
Rules
Code
Generator
Backend
Questionnaire
Models
Figure 2: Architecture of the medical information system.
I can enjoy things, despite the pain.
Not at all confident Completely confident
0 6
Figure 3: Exemplary question involving a visual analogue
scale (cf. PSEQ).
can be loaded into the backend. This document en-
compasses the meta information about the question-
naire. Such meta information is used in the mobile
app and dashboard for displaying purposes and in the
rules for the rules engine to express logic. The code
generator is able to cover the requirements for the
questionnaire part of the app well. However, there are
also custom parts which have been realized by cus-
tom code next to the generated code. For instance,
the implementation for the assessments and exercises
were too specific to our use case, thus, preventing
a meaningful abstraction into language elements for
the QuApp language. Nevertheless, the custom im-
plementations are also based on the mentioned ques-
tionnaire metadata and rules logic. Thus, they do not
pose a limitation towards our goal of making changes
easy for health professionals.
4 PROTOTYPE DEVELOPMENT
Given the requirements and software architecture out-
lined in the previous section, this section gives more
details on the development of the different system
components. First, Subsections 4.1 to 4.4 deal with
the two UI components (mobile app, dashboard) and
the components realizing the API service (backend,
rules engine). Based on this understanding of the pro-
totype, in the last Subsection 4.5, we describe how we
used our QuApp DSL to generate certain aspects of
the system automatically. Exemplary code showcas-
ing our use of the DSL and DRL rules can be found
in a dedicated GitHub repository
4
.
4.1 Mobile App
By using the mentioned JavaScript framework React
Native, the mobile app could be realized as a cross-
platform app. Hence, it can be run on both Android
and iOS devices. React Native leans on the JavaScript
library React
5
and, thus, the UI appearance and be-
havior of an app is implemented through React com-
ponents. Here, a component represents a bundle of
code that can be reused to compose the overall app
(e.g., an input element that is needed on different
screens). At runtime, React Native translates the Re-
act components to native view elements for the re-
spective mobile platform.
Once logged in, the user is presented the app’s
main screen. As depicted in Figure 4a, this screen
contains a tab bar at the bottom. Here, the user is able
to switch between four different sub-screens.
Profile. This screen contains options to view and edit
the information of the user profile. Additionally, the
user can logout from the app.
Questionnaires. Here, a list of available question-
naires is shown. After choosing a questionnaire, the
patient is presented its content step-by-step. A ques-
tionnaire is divided into sections where each section
contains questions and optionally information pages.
An information page can be used to display instruc-
tions before questions. For instance, we use informa-
tion pages to explain when a following block of ques-
tions refers to the same overall topic (e.g., about the
physical activity done in the last seven days).
All required question types mentioned previously
have been implemented. An example can be seen in
Figure 4b. Here, the input for a VAS has been real-
ized as a slider. The other question types look sim-
4
https://github.com/wwu-pi/ankle-rehab-examples
5
https://reactjs.org
A Medical Information System for Personalized Rehabilitation after Ankle Inversion Trauma
323

(a) Overview list with avail-
able questionnaires.
(b) VAS input within a ques-
tionnaire realized as a slider.
(c) Exercise instructions.
Figure 4: Exemplary features of the mobile app.
ilarly. While for single-choice questions radio but-
tons are displayed, we use check-boxes for multiple-
choice questions. Finally, for open-ended questions,
a text input field is provided.
Exercises. Analogously to the aforementioned ques-
tionnaires list, the patient is presented a list of avail-
able exercises from the homework collection. Once
an exercise has been selected, a corresponding exer-
cise screen is shown (cf. Figure 4c). Here, instruc-
tions on how to do the exercise correctly are given.
After doing the exercise, the patient can mark it as
“completed” and evaluate whether it was too difficult,
too easy, or exactly right.
From the exercise list, the patient also has the option
to access the assessments screen (e.g., in case the ex-
ercise list is still empty because pending assessments
have to be done). The patient can choose from a list of
assessments and is given instructions on how to do the
exercise or test that is going to be assessed. Further-
more, questions are shown similar to questionnaires
(cf. Figure 4b). The question types used for assess-
ments are single- and multiple-choice as well as open-
ended.
Information. The final screen provides general in-
formation for the user. Again, a list is used to display
multiple entries from which the patient can choose.
Entries are fetched from the backend as static HTML
code and are displayed accordingly when selected.
4.2 Dashboard
The UI for the dashboard is also implemented using
React components. After logging in, health profes-
Figure 5: Dashboard plot visualizing the CAIT scores for
the left and right ankle over time.
sionals get access to a list of participants. After select-
ing a participant, plots visualizing the questionnaire
scores over time are displayed. A plot with exemplary
data for the CAIT score is depicted in Figure 5. In this
case, the line plot contains two data series for the left
and right ankle. These two series correspond to two
sections in the questionnaire allowing the backend to
compute the scores individually. For other question-
naires such as the PSEQ, only a single score is com-
puted. The score calculation method is specified in
the questionnaire’s metadata.
4.3 Backend
The dashboard is bundled with the backend within a
single web application. For the backend implementa-
tion, we used the web framework Express
6
which is
6
https://expressjs.com
ICSOFT 2022 - 17th International Conference on Software Technologies
324

based on the JavaScript runtime Node.js
7
.
The main responsibility of the backend is to pro-
vide an API for the other system components. This
includes endpoints for authentication and data man-
agement.
Endpoints for data management provide the
means to read, insert, update, or delete entities in the
database. For instance, questionnaire metadata is re-
trieved by the mobile app for data collection and by
the dashboard for data visualization. Similarly, the
mobile app sends answers to questionnaires to the
backend via a corresponding endpoint.
In addition to obtaining data from the database,
certain endpoints require evaluating rules. For in-
stance, this is the case after a questionnaire or an as-
sessment has been submitted. Additionally, the rules
engine is consulted when the user evaluates the dif-
ficulty of an exercise. Finally, the rules engine deter-
mines which exercises are returned by the backend for
the homework collection.
4.4 Rules Engine
As mentioned earlier, the rules engine was imple-
mented based on the BRMS Drools. It offers an API
for the backend to trigger a rule evaluation based on
the user’s inputs. Hereby, the rules engine is com-
pletely stateless and only depends on the rules loaded
upon start and information provided in a particular re-
quest. Since Drools is implemented in Java, we also
realized the API service of the rules engine with Java
based on the Spring Framework
8
.
The rules are organized in several rule files each
containing a set of rules. Firstly, the assignment of
exercises to groups, the difficulty levels as well as the
priorities of exercises are defined using rules. Sec-
ondly, there are rule sets for evaluating which exer-
cise to add to the homework collection given a spe-
cific questionnaire or assessment input.
In Listing 1, an exemplary rule in DRL syntax
is shown. After the definition of the rule’s name in
line 3, there are two main blocks. While the when-
block (cf. line 4 ff) specifies the conditions for the
rule to fire, the then-block (cf. line 10 ff) contains
the logic to be executed when the conditions are met.
In this example, the rule is only fired when the VAS
input for the fifth question of the CAIT questionnaire
has a value higher than zero. In this case, an exercise
with ID B2 contained in exercise group G1 is added to
the list of exercises defined in line 1.
7
https://nodejs.org
8
https://spring.io
1 global List < Ex ercise > exerc i s es ;
2
3 rule " R1"
4 when
5 Question n a i r e (
6 questionna i r e I d . equa ls ( " CAIT " ) ,
7 questionnaireAnswer s . get ( " Q5")
8 > 0
9 )
10 then
11 Exerc i se e = new E x ercise () ;
12 e. s e t ExerciseId ( " B2 " ) ;
13 e. s etGroupI d (" G1 " ) ;
14 exerc i s es . add ( e ) ;
15 end
Listing 1: Exemplary rule in DRL syntax defining which
exercise to add to the homework collection based on
questionnaire inputs (simplified).
When the backend makes a request to the rules en-
gine providing the questionnaire input, the API con-
troller feeds the supplied data as facts to the working
memory of Drools. Additionally, the global variable
exercise (cf. line 1) is initialized with an empty list.
Then, all rules are fired which causes Drools to eval-
uate the rules based on the provided facts and execute
the rule logic where conditions are met. At this stage,
all applicable rules write their corresponding exer-
cises to the global variable. Subsequently, the con-
troller can return this list as a result to the request. The
backend, on the other hand, can then use the specified
IDs to obtain the exercise entities from the database
to provide them to the mobile app.
4.5 Domain-specific Language
In this subsection, the main concepts of the QuApp
DSL are presented. We developed the DSL us-
ing the Xtext
9
language workbench. After defining
the language elements with a grammar, Xtext auto-
matically generates a basic language infrastructure.
For instance, this includes a parser, basic validation,
and a plug-in integrating the language into Eclipse
IDE
10
. Additionally, Xtext provides an infrastructure
to implement custom code generators transforming
the DSL specifications to general-purpose code (e.g.,
JavaScript).
There are two concerns the DSL targets: specify-
ing mobile apps and questionnaires. Both aspects will
be discussed subsequently.
9
https://www.eclipse.org/Xtext
10
https://www.eclipse.org/eclipseide
A Medical Information System for Personalized Rehabilitation after Ankle Inversion Trauma
325
4.5.1 Mobile App Specification
To specify a mobile app, first, general properties have
to be defined. This includes the app’s name and ver-
sion. Furthermore, the URL to a data provider must
be set. In our case, this is the API provided by the
backend. Every generated mobile app will have a
questionnaire screen. Next to this basic feature, cus-
tom sub-screens for the tab bar (cf. Figure 4a) can be
created using the keyword CustomTab.
Listing 2 contains an exemplary specification of
a custom tab. Here, the functionalities of the infor-
mation screen mentioned in Subsection 4.1 are de-
fined. First, a data model for the static information
fetched from the specified API endpoint is created.
Based on the defined attributes, an index screen for
a list of multiple entities and a content screen shown
when selecting a single entity is specified. Here, the
model’s attributes are referenced. The name field is
used as a title for the list entries and the data con-
tained in the text field is handled as HTML code
and rendered accordingly. Lastly, using the keyword
InitialScreen the first screen shown after selecting
the corresponding tab bar button is defined. Besides
the shown HTMLBlock, there are other components
that can be used to display the data of an attribute on
a content screen (e.g., Text, Image, or Video).
1 CustomTab I n f o rmation . .. {
2 Model S t a ticInfo {
3 id
4 na me
5 te xt
6 }
7 FetchPath /"staticInfo"
8 fetchAsList from
9 /"staticInfo/list"
10 identifier
11 Static I n fo . id
12 IndexScreen I n f oIndex ... {
13 Title S t a ticInfo . name
14 DetailScreen I n f oConent
15 }
16 ContentScreen I n f oConent ... {
17 HTMLBlock bind S taticInf o . t ext
18 }
19 InitialScreen I n f oIndex
20 }
Listing 2: Exemplary specification of a custom tab
(simplified).
4.5.2 Questionnaire Specification
The implemented system expects the metadata for
questionnaires to be defined in a specific JSON
schema. While this format is well suited for imple-
menting application logic, it is not easy and concise
to write for a user. Consequently, we use the DSL to
specify questionnaires and generate the correspond-
ing JSON document automatically.
In Listing 3, the main structure of a questionnaire
specification is shown. After defining the question-
naire’s ID and name, a rule for the score calculation
must be set. With sumSection, the score corresponds
to the sum of the scores within a section. When mul-
tiple sections are defined, multiple scores are calcu-
lated. Another calculation method is sumAll where
only one score for all sections is determined. For each
section, an ID and name must be set and within the
section, questions and information pages are defined.
1 Questionnaire CAIT "Cumberland Ankle
2 Instability Tool"
3 CalculationRule s u m Section
4 Description "Dear patient..."
5
6 Section left "Left ankle"
7 Description "The following questions
8 concern your LEFT ankle..."
9
Question(s) / information page(s)
10
Additional section(s)
Listing 3: Exemplary questionnaire specification.
To define an information page, only an ID and the
text to display need to be specified. Question defini-
tions, on the other hand, entail more properties. For
each of the question types implemented in the mo-
bile app (cf. Subsection 4.1), a keyword is defined in
the DSL. In Listing 4, a multiple-choice question is
specified. Here, each option is assigned an individual
score. Single-choice questions can be defined anal-
ogously using the SCQuestion keyword. However,
for single-choice options, the user can define cross-
references to a follow-up question. For instance, one
could append the expression “=> S2.Q11” to line 4 to
indicate that when choosing this option the next ques-
tion will be question 11 from section 2. Without such
a cross-reference, questions are shown according to
the order in which they are defined within a section.
1 MCQuestion Q1 "I have pain in my
2 ankle."
3 Choice "Never"
4 Score 5
5 Choice "During sport"
6 Score 4
7 ...
Listing 4: Exemplary multiple-choice question (cf. CAIT).
Listing 5 contains an exemplary slider question,
i.e., a question with a VAS input. Besides defining the
titles for the two opposing categories, the minimum
and maximum values as well as the interval to use for
the slider must be set.
ICSOFT 2022 - 17th International Conference on Software Technologies
326

1 SliderQuestion Q1 "I can enjoy things
2 despite the pain."
3 MinValue 0 : "Not at all confident"
4 MaxValue 6 : "Completely confident"
5 Interval 1
Listing 5: Exemplary slider question (cf. PSEQ).
Finally, an example for an open-ended question is
shown in Listing 6. The input provided to this ques-
tion type is handled as plain text and, thus, is not con-
sidered for the score calculation.
1 OpenEndedQuestion Q26 "During the
2 last 7 days, how much time did
3 you usually spend sitting on a
4 weekday?"
5 InputText "Hours per day"
Listing 6: Exemplary open-ended question (cf. IPAQ).
5 DISCUSSION
In this section, we evaluate and discuss the results of
our work. Subsection 5.1 deals with unit and per-
formance tests evaluating the system’s conformance
to the functional requirements and its responsiveness.
Then, we assess the usability of the dashboard and the
approach of expressing expert knowledge using DRL
rules. In Subsection 5.3, we evaluate the effectiveness
of the DSL-based approach by comparing how much
lines of code (LOC) could be generated automatically
based on manually written DSL code. Lastly, we dis-
cuss limitations of the prototype.
5.1 Unit and Performance Tests
During development of the prototype, we did some
functional testing via unit tests. On the other hand,
we also did non-functional testing evaluating whether
the interaction of the different components introduces
an unacceptable latency. For instance, we measured
the mean response time of the rules engine’s API end-
points given exemplary data. Furthermore, we tested
whether large amounts of documents (up to 100,000)
in the database lead to an unacceptable increase in la-
tency when querying data within the backend’s im-
Table 1: LOC comparison between manually written and
automatically generated code for different types of models.
Model Type Written Generated
PSEQ questionnaire 44 136
IPAQ questionnaire 79 328
CAIT questionnaire 191 597
App with two custom tabs 93 1,706
Sum 407 2,767
plementation. In all cases, we did not observe un-
acceptable response times. The API endpoints re-
sponded within less than 11 ms, while the queries
took less than 200 ms. All measurements were done
on consumer-grade hardware which suggests that run-
ning the software on a server in production should
result in even lower values. Also, we checked how
long it takes to display the dashboard plots for large
amounts of data points (up to 400) which did involve
rending times of less than 34 ms.
5.2 Usability Tests
For assessing the usability of the system we con-
ducted two usability tests based on the system usabil-
ity scale (SUS) (Brooke, 1996). While the first test
concerned the dashboard’s usability (5 participants),
the second test assessed the usability of DRL rules
format (7 participants). The SUS is a questionnaire
comprised of ten statements which the participants
rate after having used the software under evaluation.
Each statement is rated on a scale between 1 (strong
disagreement) and 5 (strong agreement). In the end, a
score between 0 and 100 can be calculated after con-
verting and scaling the ratings. Here, higher scores
indicate a superior usability.
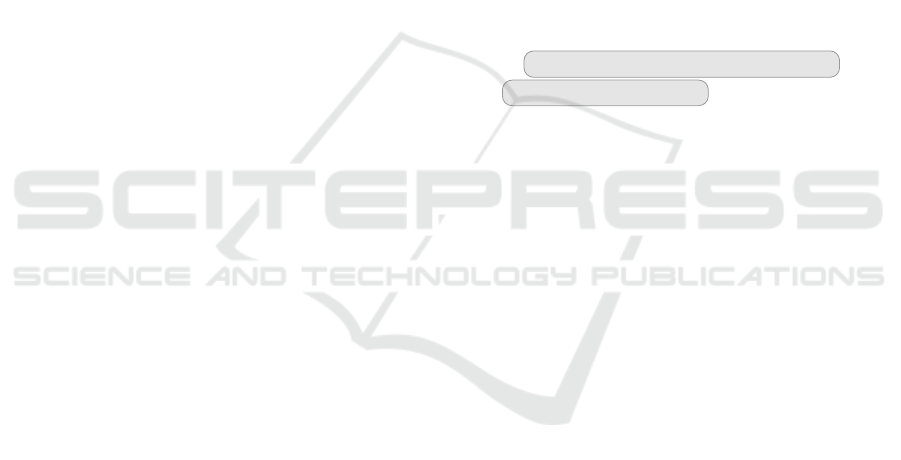
In Figure 6, the ratings for the ten statements and
for both tests can be seen. The final scores for each
participant are visualized in Figure 7. All partici-
pants had a background in medicine or physical ther-
apy and did not have prior knowledge about program-
ming. On average, the first test concerning the dash-
board resulted in a mean score of 88.57 and the sec-
ond test concerning the DRL format yielded a mean
score of 73.00. These results can be interpreted based
on the adjective rating scale suggested by Bangor et
al. (2009). The dashboard’s mean SUS score indi-
cates an “excellent” usability and the DRL format al-
most reached the rating “good”.
5.3 Lines of Code Comparison
To assess the effectiveness of the approach of defin-
ing questionnaires and parts of the mobile app based
on the QuApp DSL, we compared the LOC that had
to be written in the DSL specifications manually with
the LOC that resulted out of the code generation pro-
cess. In Table 1, the results are summarized. We
defined models of different types. Besides different
models defining questionnaires, our test also included
the specification of a mobile app with two custom
tabs. In total, based on 407 manually written LOC
2,767 LOC could be generated.
A Medical Information System for Personalized Rehabilitation after Ankle Inversion Trauma
327
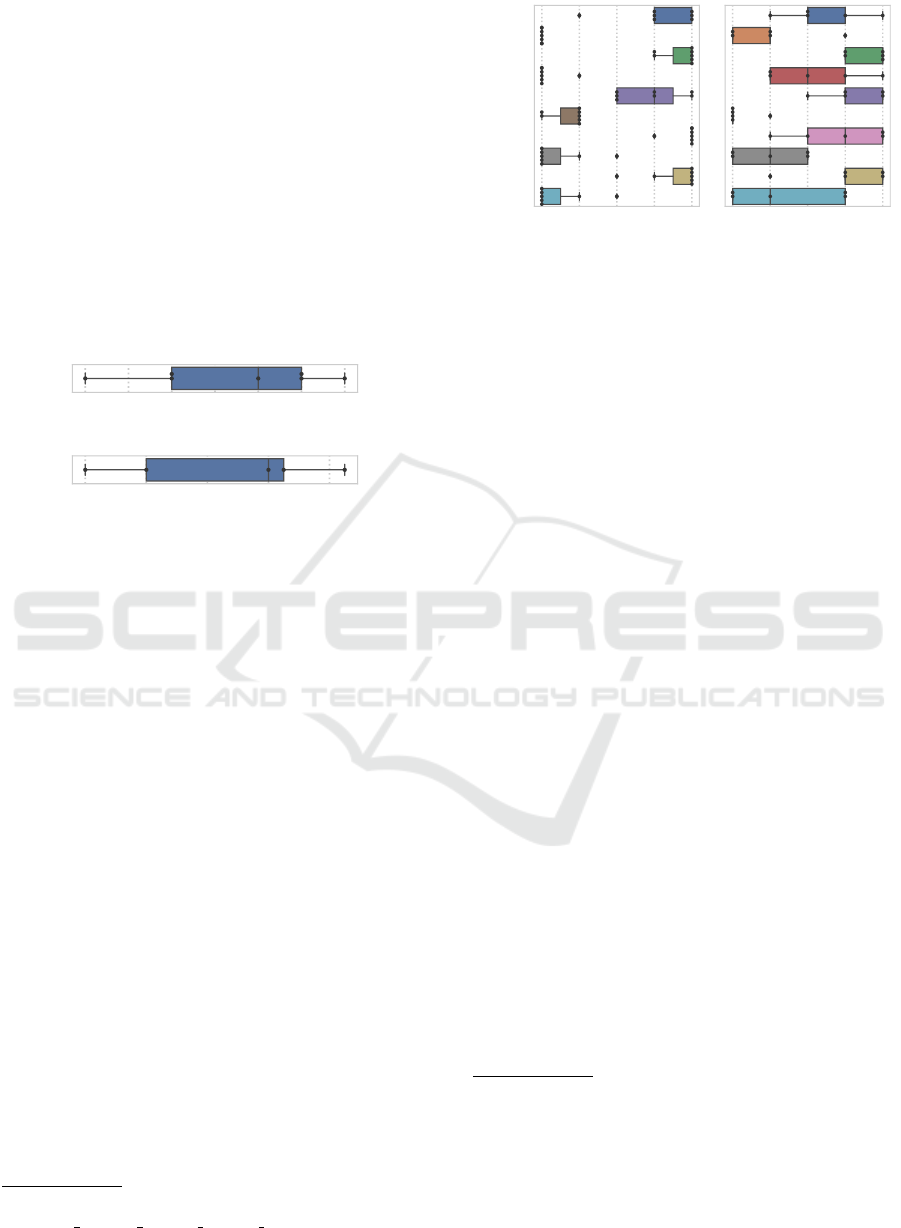
1 2 3 4 5
1. I think that I would like to use this system frequently.
2. I found the system unnecessarily complex.
3. I thought the system was easy to use.
4. I think that I would need the support of a technical person to be able to use this system.
5. I found the various functions in this system were well integrated.
6. I thought there was too much inconsistency in this system.
7. I would imagine that most people would learn to use this system very quickly.
8. I found the system very cumbersome to use.
9. I felt very confident using the system.
10. I needed to learn a lot of things before I could get going with this system.
1 2 3 4 5
1. I think that I would like to use this system frequently.
2. I found the system unnecessarily complex.
3. I thought the system was easy to use.
4. I think that I would need the support of a technical person to be able to use this system.
5. I found the various functions in this system were well integrated.
6. I thought there was too much inconsistency in this system.
7. I would imagine that most people would learn to use this system very quickly.
8. I found the system very cumbersome to use.
9. I felt very confident using the system.
10. I needed to learn a lot of things before I could get going with this system.
(a) Ratings concerning
the dashboard (n = 7).
1 2 3 4 5
(b) Ratings concerning
the DRL format (n = 5).
Figure 6: Box plots visualizing the ratings for the SUS statements.
80.0 82.5 85.0 87.5 90.0 92.5 95.0
(a) Scores concerning the dashboard (n = 7).
50 60 70 80 90
(b) Scores concerning the DRL format (n = 5).
Figure 7: Box plots visualizing the SUS scores.
5.4 Limitations
There are some limitations to our prototype. First,
the SUS score obtained for the DRL format suggests
that its usability can still be improved. One reason for
this assessment could be that still some technical un-
derstanding is needed to implement DRL rules. For
instance, in the example in Listing 1, a health profes-
sional has to understand that a global variable is to be
filled with exercises as part of the rule’s logic. One
way to overcome this limitation is to abstract away
the technical details by defining a simpler language
closer to this use case. Drools offers functionalities to
define transformations from such custom languages to
DRL constructs
11
. Furthermore, only the basic ques-
tion types required for our use case have been im-
plemented. This could be extended. Also, the gen-
erated metadata is specific to our application. One
could consider implementing (partial) compatibility
with a metadata standard such as ODM-XML
12
. This
standard can be used to specify questionnaires and is
widely supported in various tools used for clinical re-
search.
11
https://docs.drools.org/7.67.0.Final/drools-
docs/html single/# domain specific languages
12
https://www.cdisc.org/standards/data-exchange/odm
6 RELATED WORK
Examples of e-health solutions for musculoskeletal
related disorders are the mobile app or web-based sys-
tems ViViRa
13
, eCovery
14
, and Injurymap
©15
. These
systems provide a video-based intervention support.
Other systems such as MeineReha
®16
, SWORD
HEALTH
17
, Companion
®
patella
18
and Kaia
19
ad-
ditionally incorporate technical devices such as the
mobile phone’s camera and motion sensors, to eval-
uate and monitor the patient’s movements or to pro-
vide direct feedback. So far, the entrance level for
the exercises and advancement through the exercises
is mostly determined by a health professional after
personal contact (Companion
®
patella, MeineReha
®
)
or after a remote consult by means of an interac-
tive platform (SWORD HEALTH). eCovery, Kaia,
ViVRa and Injurymap
©
use a few questions or two-
dimensional video analysis with which they are able
to perform some form of a remote assessment and
monitoring of the patient’s health status. In addi-
tion, a rules based AI system has been included to
advance through the exercises (Injurymap
©
, ViViRa)
or correct exercises (Kaia). Information concerning
the disorder such as the rehabilitation process and
advice to handle pain, has been provided by a few
systems (Injurymap
©
, eCovery, Kaia, Companion
®
patella) or can be gained through chatting remotely
(SWORD HEALTH). First clinical trials with patients
suffering from an acute lateral ankle sprain (with-
13
https://www.vivira.com/
14
https://ecovery.de
15
https://www.injurymap.com
16
https://www.meinereha.de
17
https://swordhealth.com
18
https://www.medi.de/digitale-anwendungen/diga-
companion-patella
19
https://kaiahealth.com
ICSOFT 2022 - 17th International Conference on Software Technologies
328

out control groups) and user experience studies in-
dicate that users are satisfied with the app, but exer-
cise adherence may be low if patients need to exer-
cise independently (Injurymap
©
) compared to daily
remote biofeedback sessions with a health profes-
sional (SWORD HEALTH) (Bak et al., 2022; Correia
et al., 2021). Although reminders are offered by most
systems, other features such as gamification which
enhance exercise motivation have not been included
yet (Croon et al., 2021). In summary, many e-health
systems still depend on (remote) interaction with a
health professional, monitoring and feedback, the sys-
tem may require costly additional equipment, infor-
mation concerning the disorder is limited and person-
alized entrance level and advancement through the ex-
ercises is only based on rules engines in a few sys-
tems. On the contrary in our system FEAL, the per-
sonalized entry level is based on extensive question-
naires as well as an assessment with feedback from
the patient. Extensive information concerning the in-
jury is provided. Furthermore, our system does not
need additional technology and can be easily adapted
by a health professional if needed. Since the App can
store health related data such as patient’s function and
activities as well as answers from questionnaires, it
will also be a useful tool for research.
7 CONCLUSION AND OUTLOOK
Considering that ankle sprains are a frequently occur-
ring injury, this paper dealt with developing FEAL,
a medical information system for personalized reha-
bilitation after ankle inversion trauma. After giving
some medical background on this use case, we pre-
sented requirements and a software architecture for
the system. Then, we described how we developed a
prototype consisting of several components. A mobile
app for the injured person is used to obtain insights on
the user’s rehabilitation based on questionnaires, ex-
ercises, and assessments. For health professionals, on
the other hand, we implemented a dashboard helping
them to monitor and adapt the rehabilitation progress.
As part of the backend components, we developed
a rules engine allowing to recommend exercises to
the user based on the input to the mobile app. Ad-
ditionally, we introduced our DSL QuApp allowing
to specify questionnaires and mobile apps and gener-
ate corresponding code automatically. We evaluated
our work regarding different aspects (e.g., functional
conformance, performance, usability), discussed lim-
itations, and also pointed out related work.
Future work for FEAL should primarily focus on
improving usability and generalizability. We men-
tioned several means to overcome the limitations of
our approach: (1) using a customized language for
specifying Drools rules and (2) implementing com-
patibility with a metadata standard for questionnaires.
REFERENCES
Bak, J., Thorborg, K., Clausen, M. B., Johannsen, F. E.,
Kirk, J. W., and Bandholm, T. (2022). Using the
app “injurymap©” to provide exercise rehabilitation
for people with acute lateral ankle sprains seen at the
hospital emergency department – a mixed-method pi-
lot study.
Bangor, A., Kortum, P., and Miller, J. (2009). Determin-
ing What Individual SUS Scores Mean: Adding an
Adjective Rating Scale. Journal of Usability Studies,
4(3):114–123.
Bennell, K., Talbot, R., Wajswelner, H., Techovanich, W.,
Kelly, D., and Hall, A. (1998). Intra-rater and inter-
rater reliability of a weight-bearing lunge measure of
ankle dorsiflexion. Australian Journal of Physiother-
apy, 44(3):175–180.
Biørn-Hansen, A., Grønli, T.-M., and Ghinea, G. (2018).
A survey and taxonomy of core concepts and re-
search challenges in cross-platform mobile develop-
ment. ACM Comput. Surv., 51(5).
Boyer, J. and Mili, H. (2011). Agile Business Rule Devel-
opment. Springer Berlin Heidelberg.
Brooke, J. (1996). SUS: A ’Quick and Dirty’ Usability
Scale. In Jordan, P., Thomas, B., McClelland, I., and
Weerdmeester, B., editors, Usability Evaluation in In-
dustry, pages 189–194. Taylor & Francis, London.
Correia, F. D., Molinos, M., Neves, C., Janela, D., Car-
valho, D., Luis, S., Francisco, G. E., Lains, J.,
and Bento, V. (2021). Digital rehabilitation for
acute ankle sprains: Prospective longitudinal cohort
study. JMIR Rehabilitation and Assistive Technolo-
gies, 8(3):e31247.
Craig, C. L., Marshall, A. L., Sj
¨
ostr
¨
om, M., Bauman, A. E.,
Booth, M. L., Ainsworth, B. E., Pratt, M., Ekelund,
U., Yngve, A., Sallis, J. F., and Oja, P. (2003). Inter-
national Physical Activity Questionnaire: 12-Country
Reliability and Validity. Medicine & Science in Sports
& Exercise, 35(8):1381–1395.
Croon, R. D., Geuens, J., Verbert, K., and Abeele, V. V.
(2021). A systematic review of the effect of gamifica-
tion on adherence across disciplines. In Lecture Notes
in Computer Science, pages 168–184. Springer Inter-
national Publishing.
Doherty, C., Bleakley, C., Hertel, J., Caulfield, B., Ryan, J.,
and Delahunt, E. (2016). Recovery From a First-Time
Lateral Ankle Sprain and the Predictors of Chronic
Ankle Instability. The American Journal of Sports
Medicine, 44(4):995–1003.
Eils, E. and Rosenbaum, D. (2001). A multi-station propri-
oceptive exercise program in patients with ankle in-
stability. Medicine & Science in Sports & Exercise,
33(12):1991–1998.
A Medical Information System for Personalized Rehabilitation after Ankle Inversion Trauma
329

Hayes, M. H. S. and Patterson, D. G. (1921). Experimental
development of the graphic rating method. Psycho-
logical Bulletin, 18:98–99.
Hertel, J. and Corbett, R. O. (2019). An Updated Model of
Chronic Ankle Instability. Journal of Athletic Train-
ing, 54(6):572–588.
Hiller, C. E., Refshauge, K. M., Bundy, A. C., Herbert,
R. D., and Kilbreath, S. L. (2006). The Cumberland
Ankle Instability Tool: A Report of Validity and Re-
liability Testing. Archives of Physical Medicine and
Rehabilitation, 87(9):1235–1241.
Houston, M. N., Hoch, J. M., Gabriner, M. L., Kirby, J. L.,
and Hoch, M. C. (2015). Clinical and laboratory mea-
sures associated with health-related quality of life in
individuals with chronic ankle instability. Physical
Therapy in Sport, 16(2):169–175.
Nicholas, M. K. (2007). The pain self-efficacy question-
naire: Taking pain into account. European Journal of
Pain, 11(2):153–163.
Peffers, K., Tuunanen, T., Rothenberger, M. A., and Chat-
terjee, S. (2007). A design science research method-
ology for information systems research. Journal of
Management Information Systems, 24(3):45–77.
Stahl, T. and V
¨
olter, M. (2006). Model-Driven Software De-
velopment: Technology, Engineering, Management.
John Wiley.
Terada, M., Pietrosimone, B. G., and Gribble, P. A. (2013).
Therapeutic Interventions for Increasing Ankle Dor-
siflexion After Ankle Sprain: A Systematic Review.
Journal of Athletic Training, 48(5):696–709.
van Putte-Katier, N., van Ochten, J. M., van Middelkoop,
M., Bierma-Zeinstra, S. M., and Oei, E. H. (2015).
Magnetic resonance imaging abnormalities after lat-
eral ankle trauma in injured and contralateral ankles.
European Journal of Radiology, 84(12):2586–2592.
Voelter, M., Benz, S., Dietrich, C., Engelmann, B., He-
lander, M., Kats, L. C. L., Visser, E., and Wachsmuth,
G. (2013). DSL Engineering - Designing, Imple-
menting and Using Domain-Specific Languages. dsl-
book.org.
ICSOFT 2022 - 17th International Conference on Software Technologies
330
