
A Framework for T2D Management & Knowledge Discovery of
Complications in the Context of Chinese Culture: From Triggers to
Causalities
Mujiexin Liu
1
, Jianqiang Xiao
1,*
, Dazheng Zhang
2
and Zhidong Jia
3
1
Ineye Hospital of Chengdu University of TCM, Jinniu District, 610084, Chengdu, Sichuan, China
2
Chengdu University of Traditional Chinese Medicine, 610075, Chengdu, Sichuan, China
3
Chengdu Neusoft University, Qingchengshan, 611844, Sichuan, China
Keywords: Type II Diabetes Management, Symptoms, Patterns, Complications, Correlations, Knowledge Discovery.
Abstract: Background: With the ever-increasing number of Type-2 Diabetes (T2D) patients and its mortality rate in
China, the medical care system is under huge pressure with all other related complications in the world's
largest population. Failing to afford the needed resources on T2D management after patients leaving the
hospital, the burden and challenges of diabatic complications have become more acute than ever. In the
context of the Chinese culture, especially the habits and priority of eating in the daily life makes it even harder
for T2D patients to control and manage. Limited knowledge of complications and their causalities are the
biggest challenges faced by doctors all around the world. Only with the knowledge on the progression and
evolution of T2D and its complications can doctors have the opportunity to find solutions. To tackle this
daunting challenge, a system is in urgent need that can collect the real-time, patient-generated data which will
unveil the patterns about the triggers and causalities for better decision-making and, in the long run, provide
an overarching understanding of the progression and evolution of T2D and its complications.
Methods: To systematically place the data in the hands of patients, knowledge discovery based on data mining
for the proposed framework can be of very high feasibility and accuracy. The triggers, anomalies in patients'
daily life, remind patients to provide the related data input for the analysis of the risk factors, patterns, and
causalities of complications in the progression of T2D. Behind the triggers, the related known symptoms
correlated with the internal organs, are classified by their severity and locations in bodies. Distant-aid like first
responders will be arranged if very high-risk factors occur. Auto responses of suggestions will be given to
patients if the condition is not urgent. The discovered patterns and causalities will be stored in the knowledge
pool for future research and medicine development.
Results:
1. The associations between and among the internal organs brought about by the patterns behind the triggers
under urgent and non-urgent situations will give us answers to the current puzzles of the end-stage
complications.
2. Supported by the updates of patient-provided data on the anomalies going on in their bodies, the data mining
output of the correlation between internal organs and different complications can be of high accuracy with the
"1 to 1", "1 to n" and "n to 1" relationships between symptoms and organs, organs and organs.
3. The collected symptoms correlating to the pathological changes of each individual internal organ can reshape
our understanding about the functions of their own and as a part of the whole system of the human body.
4. The patterns of the known and newly discovered complications and their causalities will help doctors gain
an overarching understanding of the progression and evolution of T2D and its complications.
5. The discovered knowledge will help doctors anticipate the upcoming progressions of diseases at an expert
level with the level of comprehension well beyond the individual physician’s practice experience.
Conclusions: With the application of this framework to the management of T2D and other chronic diseases for
different groups of users, its knowledge pool will be continually enriched and enlarged. Its scalability on
diseases and causalities will probably change many current definitions and enlarge the boundary of medical
science.
554
Liu, M., Xiao, J., Zhang, D. and Jia, Z.
A Framework for T2D Management Knowledge Discovery of Complications in the Context of Chinese Culture: From Triggers to Causalities.
DOI: 10.5220/0011374200003438
In Proceedings of the 1st International Conference on Health Big Data and Intelligent Healthcare (ICHIH 2022), pages 554-564
ISBN: 978-989-758-596-8
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
1 INTRODUCTION
Type-2 Diabetes (T2D) and its ineffective
management have been challenging the health of a
very large population in China. By the figures given
in the IDF Diabetes Atlas Ninth edition 2019,
approximately 463 million adults (20-79 years) had
been living with diabetes; by 2045 this will rise to 700
million. According to the most recent study of the
prevalence of T2D in mainland China, by the standard
of HbA1c ≥6.5%, the average percentage of
diagnosed and premature T2D has reached 12.8%,
which means almost half of the adult population
suffer from the dysfunction of the glucoregulatory
system with a fast-growing tendency after age 50. (Li,
et al., 2020) The total number of people with T2D has
reached about 1.164 million in China, the largest in
the world. The percentage of diabetes among people
above 60 has reached more than 20% by 2016. (Yang,
Lu, Weng, et al. 2010) With the obesity rate for adults
over 18 already at 11.9% in 2015, the harm of
hyperglycemia goes on before the premature stage till
the occurrence of all kinds of end-stage complications
related to cardiovascular diseases, microangiopathy,
cancer, stroke, Alzheimer's disease, and depression.
(Report on nutrition and chronic diseases of the
Chinese population 2015, Chinese Medical
Association, Diabetes Branch 2018) Proportion of
microalbuminuriax, macroalbuminuria, and renal
failure in patients with T2D nephropathy has reached
25.26%, 4.34%, and 7.03% respectively. 14.9% of the
patients suffer from retinopathy while 24.05% have
diabetic peripheral neuropathy. (ADA 2019) 10.56%
of all patients who went through peripheral artery
disease tests (PAD tests) such as Ankle-Brachial
Index (ABI), angiograms, ultrasound, or MRI got
diagnosed with peripheral artery disease. (ADA
2019) Out of 33.9% of patients with cardiovascular
disease, 94.9% put up with atherosclerotic
cardiovascular disease (ASCVD). (Hong, Mosenzon,
Alguwaihes, Arenas Leon, et al. 2020) All these
problems pose a huge burden to the health system and
great risks to the wellbeing of T2D patients.
T2D management is the crucial part of the whole
course of prevention, intervention and treatment of
complications rather than just screening for the end-
stage ones. At present, insulin administration is the
main treatment for T2D patients, when
hyperglycemia cannot be controlled through diet,
exercise, and oral medication. (Kavakiotis, Ioannis,
Tsave, Olga, Salifoglou, Athanasios, Maglaveras,
Nicos, Vlahavas, Ioannis, Chouvarda, Ioanna 2017)
But according to Research Report on Burden of
Injection and Administration of Diabetic Patients,
90% of patients around the world who administer
daily injections think this therapy is impacting their
normal way of life; 72% think the inconvenience of
injection has a negative effect on following doctor's
orders; 32%
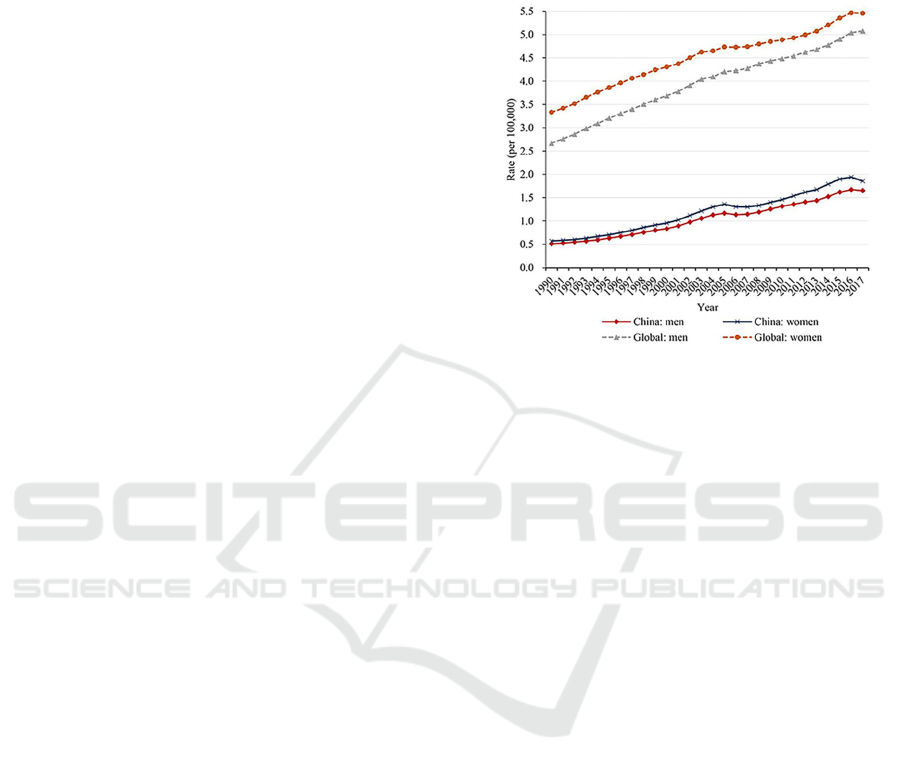
Figure 1: Prevalence of diabetes in China and around the
world from 1990 to 2017. Credit: Xiaoxue L, Chuanhua Y,
et.al. Trends in the Incidence and Mortality of Diabetes in
China from 1990 to 2017: A Joinpoint and Age-Period-
Cohort Analysis. CMR: crude mortality rate; ASMR: age-
standardized mortality rate.
gave up injection therapy because of the
inconvenience. (IQVIAA Study of the Burden of
Administration Modalities in Patients with Injectable
Hypoglycemia.) Similar problems exist among T2D
patients in China. According to a one-year cohort
study by He, et.al., the mean medicine preservation
rate (MPR) of T2D patients only reached 0.499 with
14.1% and 29% of discontinuations in the first month
and the first three months respectively. Only 53% of
the patients remain persistent, where the average time
to non-persistence in the study was 230.3 days. (Zhao,
et al. 2019) Apart from that, data from a survey by
Liu Xiaoxue, et.al. show that 39.1% of the
respondents reported experiencing at least one insulin
injection-related needle-stick injuries (NSIs) and
3.2% reported HBV infections while 0.9% had HCV
infection as a result of NSIs. (Liu, et al. 2020) As a
result, the prevalence of complications and mortality
have always been on the rise in China as shown in
figure 2 and 3. (Nam, et al. 2011, Ma, Ronald 2018,
Lee, Keen, Bennett, Fuller, Lu 2001))
.
Studies on the complications caused by T2D have
been few and information on their causalities is very
limited. This is mostly due to the absence of
symptom-based triggers or alarms for both patients
and doctors to get actively involved in generating data
and
feedback.
(Chaki,
Jyotismita,
et
al.
2020)
Even
A Framework for T2D Management Knowledge Discovery of Complications in the Context of Chinese Culture: From Triggers to
Causalities
555
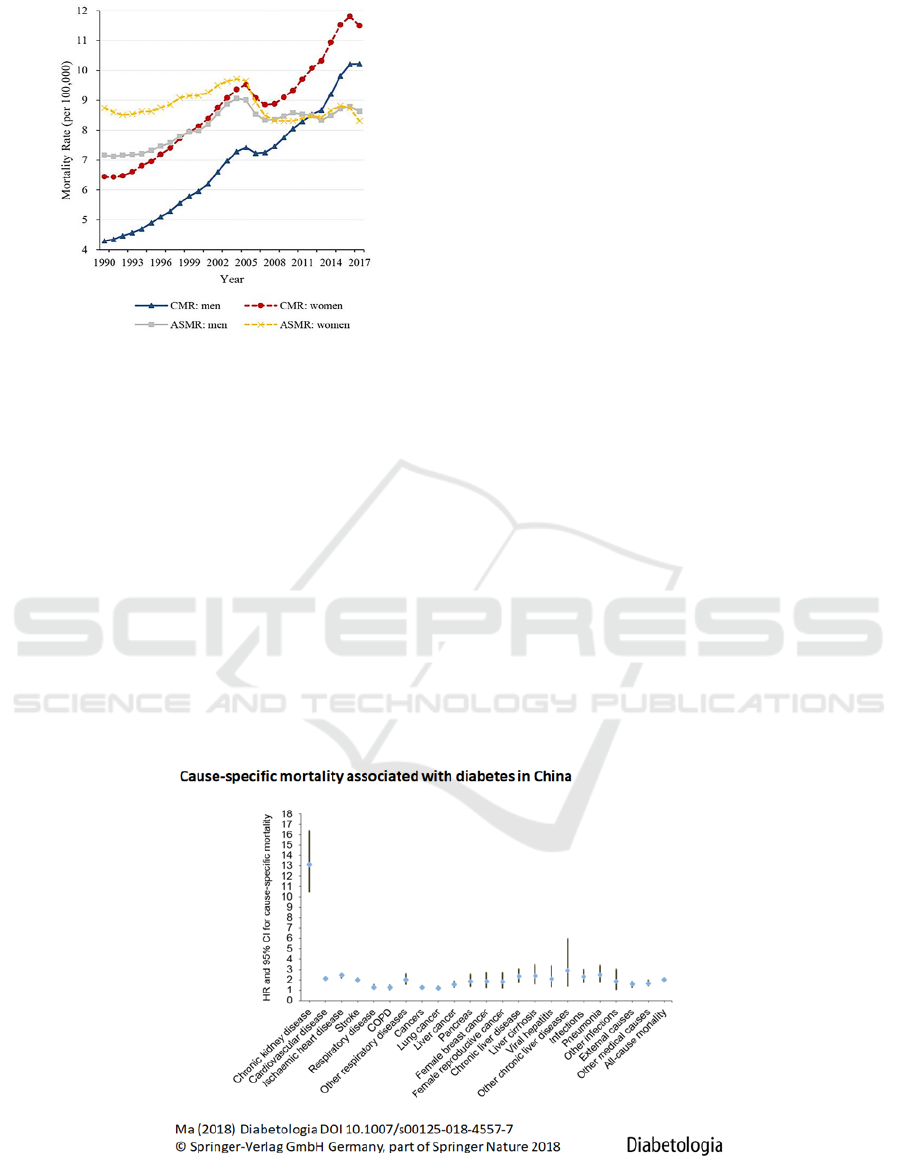
Figure 2: The mortality rate of diabetes classified by sex
groups from 1990 to 2017. Credit: Xiaoxue L, Chuanhua Y,
et.al. Trends in the Incidence and Mortality of Diabetes in
China from 1990 to 2017: A Joinpoint and Age-Period-
Cohort Analysis. CMR: crude mortality rate; ASMR: age-
standardized mortality rate.
with machine learning and artificial intelligence
applied in various products, most of them have not led
to practical solutions for real-world problems. (Yao,
Grace, et al. 2002) Without data to trace down the
correlation between T2D and internal organ's
deterioration and dysfunction going on in the course
of diabatic progression and evolution, it is hard for
doctors to make decisions or provide the needed
intervention and treatment in time. Individualized
plans and services are for sure out of the question.
Therefore, this paper aims to propose a conceptual
framework using the anomalies in patients' daily life
in correlation with the internal organs as triggers to
collect the patient-generated data in order to discover
patterns in the progression and the evolution of T2D
and its complications and form an overarching
understanding of the causalities in the context of the
Chinese culture.
2 THE CULTURAL CONTEXT OF
T2D MANAGEMENT IN CHINA
In western countries, over 75% of individuals
diagnosed with T2D receive exclusive care from
primary care providers. Yet, only about one-third of
patients correctly follow the health care provider's
directions for T2D management. (Gao, et al. 2017) In
China, doctors do a very good job educating patients
for glucose monitoring and control, food intake, and
the need for regular exercises while they are in the
hospital for deciding their dose of insulin injections
or hypoglycemic agents. It all depends on the patients
to manage and take care of themselves once they
leave the hospital. When it comes to complications,
doctors have little clue about what has caused them or
how they have developed. What's more, in the current
health care system in China with the increasing
numbers of patients and types of diseases,
overstretched doctors can spare at most 5 to 10-min
for each office visit. For patients, it is a headache just
to
think
about
the
large
crowds,
long
lines,
and
Figure 3: Cause-specific mortality rate associated with diabetes complications in China. Figure credit: Ronald C, W. Ma,
Epidemiology of diabetes and diabetic complications in China. Diabetologia 61.6 (2018): 1249-1260. Data credit: Lee ET,
Keen H, Bennett PH, Fuller JH, Lu M (2001) Follow-up of the WHO Multinational Study of Vascular Disease in Diabetes:
general description and morbidity. Diabetologia 44(Suppl 2): S3–S13.
ICHIH 2022 - International Conference on Health Big Data and Intelligent Healthcare
556

prescription. It is also expensive to stay in the hospital
for the needed adjustments or the change of
medications. For convenience, patients tend to be
easily convinced by the salespersons in pharmacies
for the promoted OTC medicines. The huge market
potential has brought about the fierce competition for
users among T2D management applications and
platforms implemented with machine learning and
AI. Unfortunately, most of the products have been
unsuccessful and costly for the mere responses on the
collected data of the glucose, blood pressure, daily
exercises rather than the real-time conditions that
T2D patients suffer from in their daily life.
(Wasserman, Jason Adam, and Brian Philip Hinote
2011).
T2D and its complications, being endemic, have
other cultural factors to be considered in the
management, which include food and dietary
preference, lifestyles, and beliefs about general
health. (Shumaker, Schron, Ockene, McBee 2004,
Diabetes Reduces the Rate of Sputum Culture
Conversion in Patients with Newly Diagnosed
Multidrug-Resistant Tuberculosis) In Chinese
culture, the freedom to enjoy food plays a critical role
in one's quality of life. (Nam, et al. 2011) Thus, the
food culture in China creates all kinds of barriers and
numerous problems for T2D patients, making it
unbelievably hard for them to handle their
management. Together with the general belief about
health in the Chinese society that patients with
chronic medical problems gradually become experts
themselves, T2D management in China is a tough war
against the limited healthcare resources, the natural
instinct, social pressure, eating habits and preference,
and the confusing information in this age of self-
media.
When we look into the food structure in China,
though the proportion of protein and vegetables has
been growing, the intake of carbohydrates has stayed
inordinate. People throughout the country start their
day with dumplings, deep-fried dough sticks,
noodles, porridge, and pancakes. Lunch is always
built upon rice or noodles. And dinner consists of
steamed bread, dumplings or pancake with porridge
and a few dishes of vegetables or pickles. What's
more, most people feel that they are never full without
a bowl of rice or noodles no matter how many dishes
they have eaten at a meal. The increasing number of
dishes on the Chinese dining tables means a
significant increase in the total amount of vegetable
oil, animal fat, sugar, and salt. Though the awareness
of a healthy life has been increasing among the whole
population, the busy life leaves little time for regular
physical exercises, which is another reason for the
increasing numbers of hyperlipidemia,
hyperglycemia, hypertension, and obesity in this
country.
Eating in China is forever the highest priority in
everyday life. Eating well is considered as the most
basic enjoyment, freedom, and the meaning of life.
Varieties on the daily menu are a must for every
family, and feasts at weekends and festivals have
been a routine. Meals for social purposes are hard to
turn down. The normality on these occasions is to
include as many good dishes as possible and the
hosts/hostesses will try their best to push people to try
everything on the table to show their hospitality.
Wine and liquor are proposed and taken as signs of
respect and gratitude to others. More will be poured
if one takes up and finishes the glass even if the
person is not good at drinking or has stated the
medical or other reasons. T2D patients have to face,
involve and interact with others on such occasions,
where it is socially unacceptable to refuse and
impossible for them to resist the good food or to
follow the strict limitations on food intake. And the
thought of just trying a little of each dish often results
in the intake of food out of the right order with
carbohydrates and energy considerably exceeding the
right amount for T2D patients.
Also, the confusing and misleading information
from the internet and peer experience make T2D
management even harder. With the general belief of
health in China, it is not hard to assume how much
more T2D patients fail to correctly follow the health
care provider's directions than the two-thirds out of
75% of patients in western countries. (Jason Fung)
Many patients tend to trust their perception when they
change their medications with over-the-counter
medicines without asking doctors for their advice
until they encounter serious troubles. To manage T2D
at the national level, the guidelines in the Treatment
and Prevention Guide for Type 2 Diabetes in China
(version 2017) on the homepage of China CDC give
clear directions: 1) collecting data about the patients'
condition, knowledge, behaviors, and psychology; 2)
pinning down the problems; 3) making plans for
management and treatment; 4) providing the planned
individual service; 5) giving feedback for adjusting
the plan. To put these jobs down to earth, we need to
pin down the triggers, find patterns supported with
valid data about the causalities and evolutions of all
diabetic complications.
A Framework for T2D Management Knowledge Discovery of Complications in the Context of Chinese Culture: From Triggers to
Causalities
557

3 TRIGGER ANALYSIS FOR T2D
MANAGEMENT
In the context of this culture, it is obvious that most
of the diseases and anomalies are the consequences of
the unregulated food structure and intake. There are
too many variables to consider if we require patients
to provide the details of their daily meals. And it is
really hard to give the right directions on what and
how much exercise to take without the information of
patients' current physical conditions. In the course of
insulin injection treatment and T2D management,
patients tend to be numb about the physical anomalies
as long as they see that their glucose level is under
check. It is exactly these physical discomforts and
anomalies that build up the complications. Just like
other diseases, only when people feel the physical
discomfort, pain or anomalies, can they be alarmed to
ponder about the reasons or whether they should go
to the hospital. Thus, to collect such patient-generated
data on their daily problems for the knowledge
discovery about the evolution of the T2D
complications, the symptoms that can alarm the
patients and push them to turn for help should also be
recorded and used as triggers apart from the most
recent records of the glucose level and blood pressure.
Thirst
Diabetic thirst, or diabetes polydipsia, is caused
by hyperglycemia which exhausts the kidneys in
producing an excessive amount of urine and
dehydrates the patients. The odds ratio of having the
symptom of abnormal thirst is 1.37 times higher (1.17
to the power of 2) for someone with an FPG=11
mmol/L than for someone with an FPG=9 mmol/L
(all other covariates being the same). (Drivsholm, de
Fine Olivarius, Nielsen, & Siersma, 2005) Long-term
polyuria can cause nausea, dizziness, headaches,
fainting, and eventually uremia.
Urine problems
As the consequences of food, water, and drinks,
urine problems are directly related to the
functionalities of the bladder and kidneys. Patients
with T2D, often suffer from pain and burning before,
during, and after urination; passing only a small
amount of urine after strong urges; trouble starting,
and a weak stream of urine. Apart from these
uncomfortable feelings, their urine is often with
bubbles and a strong stench. For female patients, T2D
independently increases the risk of urinary
incontinence. (Lifford, Karen, et al. 2005)
Hard stool and diarrhea
With the progression of T2D, many patients often
suffer from hard stools - as hard as pebbles
sometimes. This is not just a sign of constipation, or
only related to the bowels. The hard stool is the
outcome of a combination of factors such as dry or
inflamed digestive tracts. Apart from persistent
hyperglycemia and the history of having T2D as the
factors for diarrhea, cold and unsanitary food intake
are also a strong trigger in China. In diabetic patients,
metformin is a common cause of diarrhea. (Gould,
Milena, and Joseph H. Sellin 2009) Diabetic patients
are more likely to have associated diseases (e.g.,
celiac sprue and microscopic colitis) that present with
diarrhea as the sole complaint. (Gould, Milena, and
Joseph H. Sellin 2009) Ingested sugar-free foods that
may contain sorbitol or other agents can cause
diarrhea in T2D patients. Finally, diabetic
enteropathy can itself cause diarrhea. (Gould, Milena,
and Joseph H. Sellin 2009) Chronic diarrhea can
bring about further complications.
Sputum
Diabetes is a risk factor for active tuberculosis
(TB). (Kotlarsky, Pavel, et al. 2015) Thin and thick
mucus often fails to alert patients in China, who often
think of it as the consequence of cold weather or
smoking. On the contrary, they are not only related to
the lungs but also possibly to the whole
gastrointestinal system.
Sweat
Diabetes itself makes it hard to maintain a steady
body temperature. Excessive, insufficient sweat or
sweating at odd times are strong signs of many
complications. Hyperhidrosis is very common among
T2D patients. But it is still unclear when it occurs and
what the underlying causes and effects are on the
internal organs. Sweating speeds up the deterioration
of organs by driving T2D patients to drink and urinate
more. Abnormal sweating is one of the earliest
detectable neurophysiological abnormalities in small
fiber peripheral neuropathy. (Simpson, John 2018)
Heartbeat
T2D patients often suffer from shortness of breath,
sweating, rapid and irregular heartbeats, which are all
symptoms of heart diseases that might be directly
related to the spike of blood glucose. They may also
be directly related to sleeping, emotional and digestive
problems. Without such knowledge, people may
suspect straight away that they are suffering from
heart troubles. Recent observational studies indicate
the associations of insulin treatment with an increased
risk of developing or worsening pre-existing heart
ICHIH 2022 - International Conference on Health Big Data and Intelligent Healthcare
558

failure with higher mortality rates, but with little
evidence. (Didangelos, Triantafyllos, and
Konstantinos Kantartzis 2020)
Pains
T2D patients with difficulties in glycemic
management and following a recommended exercise
plan often have chronic pains. (Krein, Sarah L., et al.
2005) Headache is common among T2D patients due
to hypertension and hyperglycemia. Toothaches and
dental problems are high at risk when the blood sugar
is poorly controlled. T2D is also associated with
higher pain severity in people with localized
osteoarthritis. (Alenazi, Obaidat, Alshehri,
Alothman, Gray, Rucker, Waitman, Kluding 2020)
Findings by Lorenzo, et.al suggest that uncontrolled
diabetes may contribute to the development of
chronic back pain. (Rinaldo, Lorenzo, et al. 2017)
Weight changes
Insulin causes significant weight gain and may
also cause serious episodes of hypoglycemia.
(Didangelos, Triantafyllos, and Konstantinos
Kantartzis 2020) Both sharp weight gain and loss in a
short period are the results of poor control of blood
sugar. Some people with T2D regard weight gain as a
positive sign of being healthy especially when their
complexion is good. One study by French S, et.al.
demonstrated that the risk of diabetes was twofold
higher in the participants whose weight fluctuated
compared to those with stable weight or moderate
fluctuation in a short-term follow-up. (Park, Kye-
Yeung, et al. 2019)
Strong emotions
Diabetes distress is a prominent issue in people
with T2D which is associated with female gender and
comorbid depressive symptoms. It is important to
consider the relationship between diabetes distress
and depression, as we look into the significant overlap
between conditions. (Perrin, et al. 2017) When the
glucose level is out of control, people with T2D
become moody without being aware of their anger,
irritability, sadness, and aggressiveness. They don't
want to talk to people and become upset very easily,
which makes communication with others very
difficult. Having trouble concentrating or thinking
clearly makes them nervous and pessimistic. Their
low energy level often makes them very frustrated
and tired. In such a state, they need directions to
control their daily emotions. Doctors need to know
what is going on in the internal organs instead of just
taking it as a psychological issue.
Sleeping problems
T2D has shown to be associated with a higher
incidence of sleep disorders, which may be due to the
disease itself, secondary complications, or the
associated comorbidities. (Khandelwal, Deepak, et al.
2017) Both high and low blood sugar cause various
sleeping problems: having trouble falling asleep, very
shallow sleep, short sleep, and waking up at night.
Poor sleep can bring about many problems to people
with T2D, and be a very strong trigger for them to
seek solutions.
Leg swelling
Swelling in the lower body including legs, ankles,
and feet caused by a buildup of fluid in the body
(Water Retention) is a common symptom and one of
the benchmarks of T2D. Other symptoms that occur at
the same time will change our understanding of the
functions of some internal organs. Diabetic muscle
infarction (DMI) is a rare microvascular complication
of spontaneous ischemic necrosis of skeletal muscle in
patients with poorly controlled diabetes. (Seaman,
Callie, et al. 2019) As a less commonly reported
complication due to poorly controlled T2D associated
with multiple end-organ microvascular sequelae, the
occurrence of painful swelling of muscles, particularly
of lower limbs, should raise suspicion of DMI.
Increased clinical awareness is important for early
recognition, particularly in a diabetic patient
presenting with a painful thigh or leg swelling.
(Jevalikar, Ganesh, et al. 2019, Grigoriadis, et al.
2000)
These triggers, the high alerts on the physical
changes in what people with T2D can see and feel in
their daily lives, are the causes of all different kinds
of complications. They can push T2D patients to
check how serious their problems are and work much
more effectively than "motivations" just for
monitoring the blood sugar without the information
about their daily problems and the needed guidance.
As these triggers are all connected with the internal
organs, the patterns found in the future will build up
a knowledge pool that will not only navigate patients
to understand their conditions and the needed actions
but also provide the evidence for the doctors' timely
intervention, treatment, and research.
A Framework for T2D Management Knowledge Discovery of Complications in the Context of Chinese Culture: From Triggers to
Causalities
559
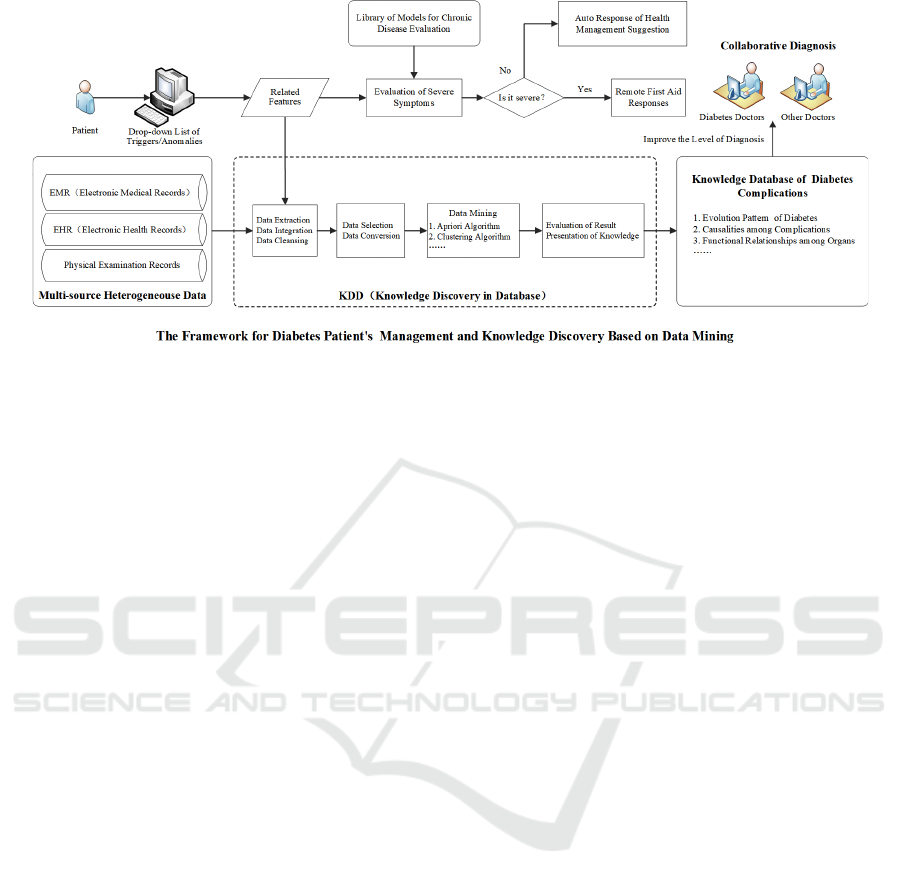
Figure 4: The framework for diabetes patient management and knowledge discovery based on Knowledge Discovery in
Database (KDD).
4 THE FRAMEWORK FOR T2D
MANAGEMENT AND
KNOWLEDGE DISCOVERY
With a patient-controlled interface, this framework
integrates patient-generated real-time data with the
EMR, EHR, and physical examination records. By
using the anomalies of T2D patients in their daily
lives as triggers, patients go through and check all
thesymptoms, correlated with the internal organs,
they are suffering at the moment. For serious cases,
patients will be required to upload related evidence
that will be analyzed by the system to support the
doctors' decision-making. If not, the system will give
suggestions on their management. The aggregation of
these data will gradually identify the risk factors for
early intervention and unveil the underlying
biological pathways of T2D complications. New
patterns and their pathologies will be captured,
analyzed by the system, and stored in the knowledge
pool, which will paint an overarching picture about
the relationships between the triggers and the
causalities on the evolution of T2D complications.
To systematically place the data in the hands of
patients, they need to log in with any of the personal
data like the name or ID number with the most recent
records of their glucose level and blood pressure. To
help patients pin down their problems quickly, the
drop-down list of the triggers in the system will
remind them of the anomalies they may have at the
moment with all the related symptoms that are used
as part of data input. When acute and severe
symptoms are marked under one trigger, patients will
be guided to check for other related symptoms and
asked to upload pictures and videos if the evidence is
needed. Even if they don't have serious physical
problems, these triggers can still serve as reminders
for them to check about their current conditions for
learning, risk management, and prevention.
Behind the triggers, the mapping of all the related
symptoms to the corresponding internal organs is the
most basic rule of this framework. The symptoms
should be classified by their severity and body parts.
All the input symptoms behind each trigger start with
the ones that are very closely related to T2D, guiding
patients to check other possible symptoms that are not
directly related but common with complications.
Many of the symptoms in one group may overlap with
those in others. For example, strong thirst, a very
common symptom of T2D, may also be caused by
xerostomia or long-term diarrhea. Weight loss,
another strong alert of T2D, may also be caused by
inflammatory bowel disease. In other words, one
symptom may trigger patients to go through many
other ones to help form the picture of the evolution of
T2D complications.
As T2D complications affect all organs, all the
input symptoms also include those of different
complications that correlate with the corresponding
internal organs. (Alicic, Radica Z., Michele T.
Rooney, and Katherine R. Tuttle. 2017) Supported by
the known symptoms and their relationships with the
internal organs, the output of data mining can be of
high accuracy. The patterns captured can be various
with the "1 to 1", "1 to n", and "n to 1" relationships
between symptoms and organs, organs and organs.
With the increase of users over time, new patterns of
T2D and the complications can be discovered and
verified. Over time, a network of disease connections
ICHIH 2022 - International Conference on Health Big Data and Intelligent Healthcare
560

can be formed for doctors, researchers and machine
learning models to learn and apply. Across the board,
all the patterns captured in the future will give us full
pathways of T2D progression and complications.
Some will fill up the gaps about the evolution of all
the known end-stage complications of diabetes
nephropathy (DN), diabetes retinopathy (DR),
diabetic foot, cardiovascular disease, and stroke. The
different stages will be clearly marked with the
corresponding triggers at different times, which link
up all the symptoms that are related to the internal
organs. The patterns of respective phases of
complications will pave the clear paths of how they
reach the final, irreversible stage.
The associations between and among the internal
organs brought about by the triggers at different times
will, first of all, give us answers to the current puzzles
of the end-stage complications. The patterns about the
retinopathy, for example, will clearly show how the
renal injury precedes retinal damage apart from the
fact that the level of renal impairment is proportional
to the level of eye damage as DR and DN has a
unidirectional correlation (Sulaiman, Mahaboob
Khan. 2019). These can help find new markers for
designing clinical trials that evaluate clinically
pertinent endpoints (e.g., glomerular hyperfiltration,
inflammation, and fibrosis) (Powell, Cooksley,
Hanson , Searle , Halliday, Powell 1988), and even
expand our knowledge on the association between
metabolic changes and DN. Some of these patterns
will help explain why the prevalence of chronic
kidney disease (CKD) in T2D patients has not
witnessed any decrease in the last two decades and
lead to the identification of additional factors in its
progression despite the aggressive blood sugar
control (Pearce, Ian, et al. 2019). Others will help
evaluate the findings with clinical manifestations
before kidney damage becomes irreversible that can
clearly show whether there is an association between
non-alcoholic fatty liver disease (NAFLD) and
progression of diabetic nephropathy (Hum Pathol
1989).
The collected symptoms correlating to the
changes of specific internal organs behind the triggers
will probably reshape our understanding of the
functions of each individual one. Here we can take the
liver for example, because it is consistently associated
with other complications of T2D with the severity of
DR linked to a higher risk of the presence of, or
developing other micro and macrovascular
complications as well as a strong predictor of stroke
and cardiovascular disease. (Itoh, Yougel, Kawagoe
1987) Apart from the answers for the prevalence of
NAFLD in diabetes estimated at 34–74% (Diehl,
Goodman, Ishak 1988, Pinto, Baptista, Camilo,
Valente, Saragoca, de Moura, Adami, Chow, Nyren,
Berne, Linet, Ekbom, Wolk, McLaughlin, Fraumeni
1996, Wanless, Lentz 1990), the emerged new
patterns will help explain why the incidence of
cirrhosis or severe fibrosis show a significant increase
with a 2.52 SMR (standardized mortality ratio) or a
6.84 SMR in the patients going through insulin
treatment (Wideroff, Gridley, Mellemkjaer, Chow,
Linet, Keehn, Borch-Johnsen, Olsen 1996). They will
also help us understand why there is a fourfold
increased prevalence of hepatocellular carcinoma in
patients with diabetes as well as an increased
prevalence of diabetes in patients with hepatocellular
carcinoma (Fujino, Mizoue, Tokui, Yoshimura 2001,
El-Serag 2004, El-Serag, Everhart 2002, Chan,
Truman, Gurwitz, Hurley, Martinson, Platt, Everhart,
Moseley, Terrault, Ackerson, Selby 2003). The
functional changes going on in the liver along the
course will give us ideas on how acute liver failure
has appeared to be increased in patients with T2D.
(Tolman, Fonseca, Dalpiaz, & Tan, 2007) Liver, with
so many overlapping symptoms with T2D such as
fatigue, mood disorders, (D’Mello, Charlotte, and
Mark G. Swain 2014) weight loss, abdominal pain,
leg swelling, bleeding, and shortness of breath, will
probably become the real culprit of T2D. Its
deterioration and dysfunction can be the cause of the
end-stage complications and the deterioration of other
organs. If liver stagnation can reveal itself through
depressive emotions, pain in the chest or flanks and a
tendency to sigh often (Wei et al. 2018), the
overlapping symptoms correlated to emotions may all
relate to liver dysfunction.
The vertical patterns behind each trigger, like the
trigger of emotions, will probably extend or even
change our boundaries of medical science. Likewise,
the patterns behind the triggers of heartbeat and
panting, which can be directly caused by
hyperglycemia, can be a strong sign of T2D
management failure rather than that of cardiovascular
diseases. And the pattern behind the trigger of urine
problems may partially explain the leg swelling
troubles of T2D patients. The changes of stool from
normal to pebbles or diarrhea may not have a direct
relationship with the underconsumption of vegetables
and fruits, or the inflammation of the bowels.
All the causalities captured by the system together
with the known relationships between the internal
organs and the known symptoms will largely cut short
the path and time on the future research for solutions.
These outcomes will far exceed the goals that past
machine learning methods tried to achieve in
medicine to help physicians anticipate future events
A Framework for T2D Management Knowledge Discovery of Complications in the Context of Chinese Culture: From Triggers to
Causalities
561

at an expert level with the information well beyond
the individual physician’s practice experience.
(Rajkomar, Alvin, Jeffrey Dean, and Isaac Kohane
2019) At the population level, the same type of
forecasting can increase the utilization of health care
services and enable the identification of patients with
chronic diseases who will soon have high-risk
conditions. (Rajkomar, Alvin, Jeffrey Dean, and Isaac
Kohane 2019)
All the patterns and causalities will be stored in
the knowledge pool for comparison with the initial
diagnosis, which will include those of the known and
newly discovered complications, the development of
one specific or one group of symptoms related to an
organ, the functional relationships between and
among organs and how they work as a whole system
in the human body. The discrepancies from the
patterns can be reviewed together by doctors for
better understanding and solution optimization. The
curated data sets with newly uploaded evidence can
be of great value for regional prescribing practices
and at the same time, relevant variables will be
automatically extracted for ease of use.
5 CONCLUSIONS
The knowledge pool will be continually enriched and
enlarged when this framework is applied to the
management of other chronic diseases like
cardiovascular disease, respiratory disease, chronic
liver disease, chronic obstructive pulmonary disease,
chronic kidney disease, cancer, arthritis, and so on.
The overlaps and relationships within each path of the
development of chronic disease symptoms and
complications can be discovered and classified, like
those of Type-2 Diabetes, for earlier intervention and
more effective management. The focus of the future
research is to look at the changes of the internal
organs vertically and horizontally at the same time.
The emerging patterns and correlations among
diseases and organs will enable future research to
become even more targeted and translatable. With a
broadened view and the support of the knowledge
discovery framework, concerted and collaborated
consultations will become much more accurate and
effective for clinical diagnosis and treatments. The
underlying relationships with the pathological
changes of the internal organs will bring about many
new insights and even broaden our view of medicine.
Most significantly, the world of the western medicine
and TCM can be bridged up for productive
collaborations and co-operations.
ACKNOWLEDGMENTS
Conflicts of interest: None declared.
Funding:
1. The design and development of an
application for the multi-wavelength retinal image
with cross-coupled structural function. Foundation
for Major Project of Scientific Instruments of
Ministry of Science and Technology of China,
2013YQ49085901
2. Research on the service model of the
National TCM Health Tourism Demonstration Zone
for Overseas Chinese. 2021SF02
REFERENCES
ADA 2019; Prevalence of Diabetic Complications in China
Adami HO, Chow WH, Nyren O, Berne C, Linet MS,
Ekbom A, Wolk A, McLaughlin JK, Fraumeni JF Jr:
Excess risk of primary liver cancer in patients with
diabetes mellitus. J Natl Cancer Inst 88:1472–1477,
1996
Alenazi AM, Obaidat SM, Alshehri MM, Alothman S, Gray
C, Rucker J, Waitman LR, Kluding PM. Type 2
Diabetes Affects Joint Pain Severity in People with
Localized Osteoarthritis: A Retrospective Study. Pain
Med. 2020 May 1;21(5):1025-1031. doi:
10.1093/pm/pnz299. PMID: 31710675; PMCID:
PMC7209370.
Alicic, Radica Z., Michele T. Rooney, and Katherine R.
Tuttle. "Diabetic kidney disease: challenges, progress,
and possibilities." Clinical Journal of the American
Society of Nephrology 12.12 (2017): 2032-2045.
Chaki, Jyotismita, et al. "Machine learning and artificial
intelligence-based Diabetes Mellitus detection and self-
management: A systematic review." Journal of King
Saud University-Computer and Information Sciences
(2020).
Chan KA, Truman A, Gurwitz JH, Hurley JS, Martinson B,
Platt R, Everhart JE, Moseley RH, Terrault N,
Ackerson L, Selby JV: A cohort study of the incidence
of serious acute liver injury in diabetic patients treated
with hypoglycemic agents. Arch Intern Med 163:728–
734, 2003
Chinese Medical Association, Diabetes Branch. Chinese
guidelines for the prevention and treatment of type 2
diabetes mellitus (2017 edition) [J]. Chinese Journal of
Diabetes, 2018, 10(01):4-67. DOI:
10.3760/cma.j.issn.1674-5809.2018.01.003.
D’Mello, Charlotte, and Mark G. Swain. "Liver–brain
interactions in inflammatory liver diseases:
implications for fatigue and mood disorders." Brain,
behavior, and immunity 35 (2014): 9-20.
Diabetes Reduces the Rate of Sputum Culture Conversion
in Patients with Newly Diagnosed Multidrug-Resistant
Tuberculosis
ICHIH 2022 - International Conference on Health Big Data and Intelligent Healthcare
562

Didangelos, Triantafyllos, and Konstantinos Kantartzis.
"Diabetes and Heart Failure: Is it Hyperglycemia or
Hyperinsulinemia?" Current Vascular Pharmacology
18.2 (2020): 148-157.
Diehl AM, Goodman Z, Ishak KG: Alcohol-like liver
disease in nonalcoholic: a clinical and histologic
comparison with alcohol-induced liver injury.
Gastroenterology 95:1056–1062, 1988
Drivsholm, T., de Fine Olivarius, N., Nielsen, A. B. S., &
Siersma, V. (2005). Symptoms, signs, and
complications in newly diagnosed type 2 diabetic
patients, and their relationship to glycemia, blood
pressure, and weight. Diabetologia, 48(2), 210–214.
doi:10.1007/s00125-004-1625-y
El-Serag HB, Everhart JE: Diabetes increases the risk of
acute hepatic failure. Gastroenterology 122:1822–
1828, 2002
El-Serag HB, Tran T, Everhart JE, Kaserer K, Fiedler R,
Steindl P, Muller CH, Wrba F, Ferenci P, Rubbia-
Brandt L, Leandro G, Spahr L, Giostra E, Quadri R,
Male PJ, Negro F, Hui JM, Kench J, Farrell GC, Lin R,
Samarasinghe D, Liddle C, Byth K, George J, Castera
L, Hezode C, Roudot-Thoraval F, Lonjon I, Zafrani ES,
Pawlotsky JM, Dhumeaux D, Lonardo A, Adinolfi LE,
Loria P, Carulli N, Ruggiero G, Day CP: Diabetes
increases the risk of chronic liver disease and
hepatocellular carcinoma. Gastroenterology 126:460–
468, 2004
Fujino Y, Mizoue T, Tokui N, Yoshimura T: Prospective
study of diabetes mellitus and liver cancer in Japan.
Diabetes Metab Res Rev 17:374 –379, 2001
Gao, Chenchen, et al. "Mobile application for diabetes self-
management in China: Do they fit for older adults?"
International journal of medical informatics 101
(2017): 68-74.
Gould, Milena, and Joseph H. Sellin. "Diabetic diarrhea."
Current gastroenterology reports 11.5 (2009): 354-359.
Grigoriadis, E. L. I. Z. A. B. E. T. H., et al. "Skeletal muscle
infarction in diabetes mellitus." The Journal of
Rheumatology 27.4 (2000): 1063-1068.
Hong Tianpei., et al. CAPTURE. GW-ICC 2020 Poster:
GW31 –e1199.
IQVIAA Study of the Burden of Administration Modalities
in Patients with Injectable Hypoglycemia.
https://www.iqvia.com/insights/the-iqvia-
institute/reports/economic-implications-of-improving-
type-2-diabetes-management-in-china
Itoh S, Yougel T, Kawagoe K: Comparison between
nonalcoholic steatohepatitis and alcoholic hepatitis.
Am J Gastroenterol82:650–654, 1987
Jason Fung, Complications of diabetes – a disease affecting
all organs [Web URL]
https://www.dietdoctor.com/complications-diabetes-
disease-affecting-organs
Jevalikar, Ganesh, et al. "Diabetic muscle infarction in type
1 and type 2 diabetes mellitus: lessons from two cases."
International Journal of Diabetes in Developing
Countries 39.4 (2019): 764-767.
Kavakiotis, Ioannis; Tsave, Olga; Salifoglou, Athanasios;
Maglaveras, Nicos; Vlahavas, Ioannis; Chouvarda,
Ioanna (2017). Machine Learning and Data Mining
Methods in Diabetes Research. Computational and
Structural Biotechnology Journal, 15(), 104–116. doi:
10.1016/j.csbj.2016.12.005
Khandelwal, Deepak, et al. "Sleep disorders in type 2
diabetes." Indian journal of endocrinology and
metabolism 21.5 (2017): 758.
Kotlarsky, Pavel, et al. "Link between retinopathy and
nephropathy caused by complications of diabetes
mellitus type 2." International ophthalmology 35.1
(2015): 59-66.
Krein, Sarah L., et al. "The effect of chronic pain on
diabetes patients’ self-management." Diabetes care
28.1 (2005): 65-70.
Lee ET, Keen H, Bennett PH, Fuller JH, Lu M (2001)
Follow-up of the WHO Multinational Study of
Vascular Disease in Diabetes: general description and
morbidity. Diabetologia 44(Suppl 2): S3–S13
Li Yongze, et al., Prevalence of diabetes recorded in
mainland China using 2018 diagnostic criteria from the
American Diabetes Association: national cross pal
study. BMJ 2020;369:m997 DOI: 10.1136/bmj.m997
Lifford, Karen L., et al. "Type 2 diabetes mellitus and risk
of developing urinary incontinence." Journal of the
American Geriatrics Society 53.11 (2005): 1851-1857.
Liu, Xiaoxue et al. “Trends in the Incidence and Mortality
of Diabetes in China from 1990 to 2017: A Joinpoint
and Age-Period-Cohort Analysis.” International journal
of environmental research and public health vol. 16,1
158. 8 Jan. 2019, doi:10.3390/ijerph16010158Broome,
David T., C. Beau Hilton, and Neil Mehta. "Policy
Implications of Artificial Intelligence and Machine
Learning in Diabetes Management." Current Diabetes
Reports 20.2 (2020): 5.
Ma, Ronald CW. "Epidemiology of diabetes and diabetic
complications in China." Diabetologia 61.6 (2018):
1249-1260.
Mosenzon O, Alguwaihes A, Arenas Leon J.L., et al.
CAPTURE Abstract 158. Presented at the 56th Annual
Meeting of the European Association of the Study of
Diabetes, Macrovascular complications and beyond,
10:15 CDT on 24 September 2020.
Nam, Soohyun, et al. "Barriers to diabetes management:
patient and provider factors." Diabetes research and
clinical practice 93.1 (2011): 1-9.
Nam, Soohyun, et al. "Barriers to diabetes management:
patient and provider factors." Diabetes research and
clinical practice 93.1 (2011): 1-9.
Park, Kye-Yeung, et al. "Bodyweight fluctuation as a risk
factor for type 2 diabetes: results from a nationwide
cohort study." Journal of clinical medicine 8.7 (2019):
950.
Pearce, Ian, et al. "Association between diabetic eye disease
and other complications of diabetes: implications for
care. A systematic review." Diabetes, Obesity and
Metabolism 21.3 (2019): 467-478.
Perrin, N. E., et al. "The prevalence of diabetes‐specific
emotional distress in people with Type 2 diabetes: a
systematic review and meta‐analysis." Diabetic
Medicine 34.11 (2017): 1508-1520.
A Framework for T2D Management Knowledge Discovery of Complications in the Context of Chinese Culture: From Triggers to
Causalities
563

Pinto HC, Baptista A, Camilo ME, Valente A, Saragoca A,
de Moura MC: Nonalcoholic steatohepatitis:
clinicopathological comparison with alcoholic hepatitis
in ambulatory and hospitalized patients. Dig Dis Sci
41:172–179, 1996
Powell EE, Cooksley WG, Hanson R, Searle J, Halliday
JW, Powell LW: The natural history of nonalcoholic
Rajkomar, Alvin, Jeffrey Dean, and Isaac Kohane.
"Machine learning in medicine." New England Journal
of Medicine 380.14 (2019): 1347-1358.
Report on nutrition and chronic diseases of the Chinese
population (2015) [M]. Bureau of Disease Prevention
and Control, National Health and Family Planning
Commission. Beijing: People's Health Publishing
House, 2015
Rinaldo, Lorenzo, et al. "Diabetes and back pain: markers
of diabetes disease progression are associated with
chronic back pain." Clinical Diabetes 35.3 (2017): 126-
131.
Seaman, Callie, et al. "Diabetic Muscle Infarction: A Rare
End-Organ Vascular Complication of Diabetes."
Marshall Journal of Medicine 5.4 (2019): 28.
Shumaker S, Schron E, Ockene J, McBee W. The handbook
of health behavior change. New York: Springer; 2004
Simpson, John. "Abnormal sweating in diabetes--
implications for screening for diabetic peripheral
neuropathy." Diabetic Foot Journal 21.4 (2018).
Steatohepatitis: a follow-up study of forty-two patients for
up to 21 years. Hepatology 11:74–80, 1990 Lee RG:
Nonalcoholic steatohepatitis: a study of 49 patients.
Hum Pathol 20:594 –598, 1989
Sulaiman, Mahaboob Khan. "Diabetic nephropathy: recent
advances in pathophysiology and challenges in dietary
management." Diabetology & metabolic syndrome
11.1 (2019): 7.
Tolman, K. G., Fonseca, V., Dalpiaz, A., & Tan, M. H.
(2007). Spectrum of Liver Disease in Type 2 Diabetes
and Management of Patients with Diabetes and Liver
Disease. Diabetes Care, 30(3), 734–743.
doi:10.2337/dc06-1539
Wanless IR, Lentz JS: Fatty liver hepatitis (steatohepatitis)
and obesity: an autopsy study with analysis of risk
factors. Hepatology 12:1106–1110, 1990
Wasserman, Jason Adam, and Brian Philip Hinote.
"Chronic illness as incalculable risk: Scientific
uncertainty and social transformations in medicine."
Social Theory & Health 9.1 (2011): 41-58.
Wei et al. (Wei, Y., Wang, T., Wu, H., Yamei, H., Wu, M.,
Zheng, M., Zhou, R. et al. (March, 2018). Biological
mechanisms underlying the liver’s regulation of
emotions in women: A study using the Trier Social
Stress Test. Journal of Traditional Chinese Medical
Sciences, 5(2), 110-118. doi: 10.1016/…. et al. 2018)
Wideroff L, Gridley G, Mellemkjaer L, Chow WH, Linet
M, Keehn S, Borch-Johnsen K, Olsen JH: Cancer
incidence in a population-based cohort of patients
hospitalized with diabetes mellitus in Denmark. J Natl
Cancer Inst 89:1360–1365, 1997
YangW, LuJ, WengJ, et al. Prevalence of diabetes among
men and women in China[J]. N Engl J Med, 2010,
362(12):1090-1101. DOI: 10.1056/NEJMoa0908292.
Yao, Grace, et al. "Development and verification of validity
and reliability of the WHOQOL-BREF Taiwan
version." Journal of the Formosan Medical Association
101.5 (2002): 342-351.
Zhao, Fang, et al. "Burden of insulin injection-related
needlestick injuries in mainland China–prevalence,
incidence, and healthcare costs." International journal
of nursing studies 97 (2019): 78-83.
ICHIH 2022 - International Conference on Health Big Data and Intelligent Healthcare
564
