
The Method and Apparatus for Peripheral Arterial Disease
Treatment
Alexey Sudarev
1,2
a
and Evgeny Korotich
1,2
b
1
Institute of Radio-Engineering and Electronics RAS, 11 bldg 7, Mokhovaya st., Moscow, 125009, Russia
2
CONSTEL LLC, 19 bldg. 2 st. Stromynka, Moscow, 107076, Russia
Keywords: Peripheral Arterial Disease (PAD) Treatment, Cardiosynchronized Sequential Antegrade
Pneumocompression (CSAP), Enhanced External Counterpulsation (EECP).
Abstract: The paper is devoted to a new method of peripheral arterial disease (PAD) treatment - cardiosynchronized
antegrade pneumocompression. The method is based on sequential compression of the lower extremities to
create an enhanced antegrade pressure wave in the arteries in order to increase blood flow in the distal parts
of the lower extremities. The main provisions of the method, the physiological model of exposure are
considered. It is shown how to optimally synchronize the impulses with the cardiac cycle for the
simultaneous achievement of a beneficial hemodynamic effect in the limbs and coronary vessels. The
structure of the device for the implementation of the method based on the system for external
counterpulsation CARDIOPULSAR is presented. The physiological effects of exposure (increased blood
flow, ABPI, temperature of the extremities) were investigated. The results of treatment on volunteers were
presented.
a
https://orcid.org/0000-0001-9683-1922
b
https://orcid.org/0000-0001-6805-330X
1 INTRODUCTION
Peripheral arterial disease of the lower limb arteries
(PAD) occur in 2 - 3% of the population, accounting
for more than 20% of cardiovascular diseases.
(Dormandy J. et al, Fowkes, F.G.R. et al).
Surgical treatments for PAD are widely used but
non-invasive methods are also known, including
sequential rhythmic pneumatic compression of the
lower extremities using inflatable cuffs (not
synchronized with the heart rate). In particular, the
positive experience of using pneumatic compression
in a peripheral wave mode is known (compression
levels were exceeded the systolic blood pressure on
the brachial artery by 10 - 20 mm Hg) (Lipnitsky
E.M. et al,
Delis K.T., Knaggs A.L.
). In this case the
front duration of pneumatic pulses and the delay
between successive pulses are on the order of
several seconds.
There are also known methods and devices for the
treatment of vascular diseases of the lower extremities
based on compression of the vessels of the affected
extremity with a single cuff synchronized with cardiac
activity (ECG) (Benjamin et al., Dillon RS.).
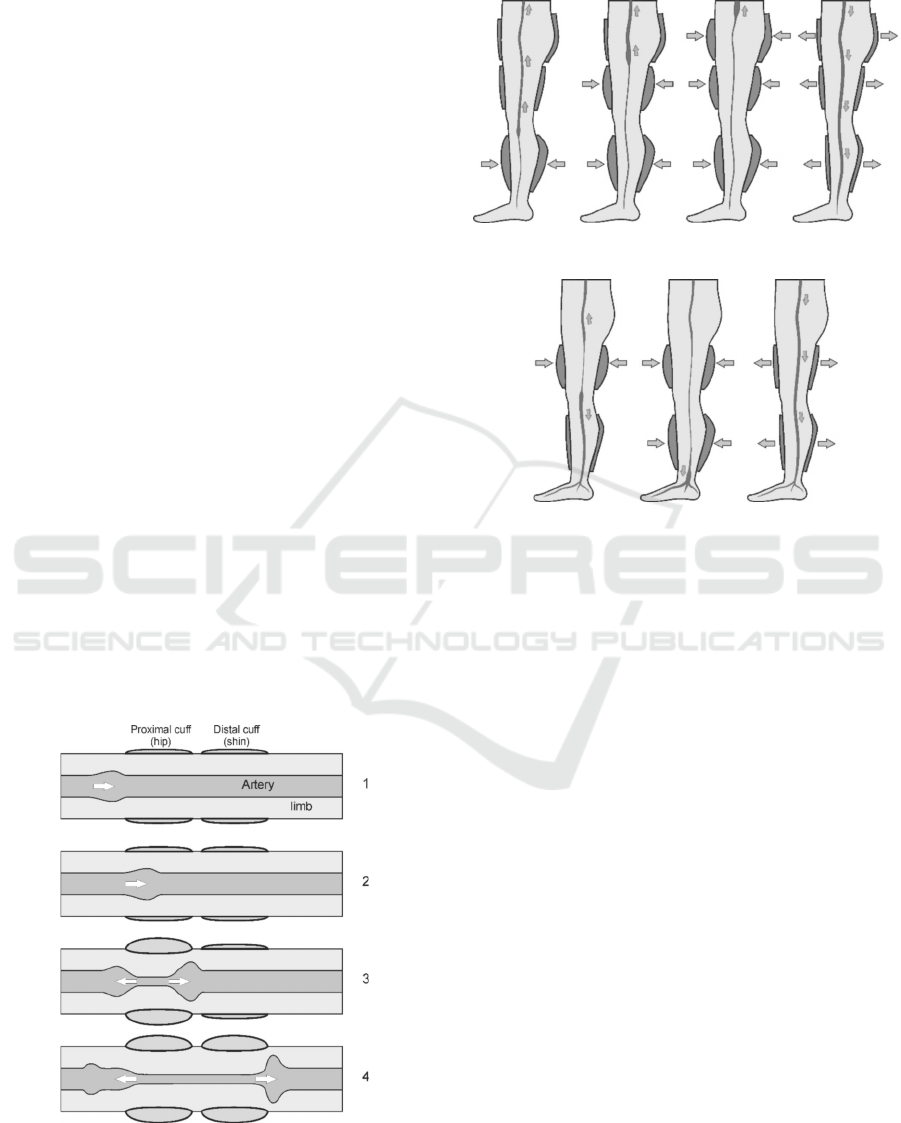
The widely used Enhanced External
Counterpulsation method (EECP) (Conti C.R) uses
separate cuffs for the shins, hips and buttocks. With
the help of successive compression in the direction
from bottom to top, a retrograde pressure wave is
effectively created in the arterial system, which
increases myocardial perfusion and a simultaneous
release of pressure in the compression cuffs of the
extremities, which reduces the systolic work.
Such an effect is capable of producing a whole
chain of favorable physiological changes in the body
(Bonetti P.O. et al). An increase in coronary blood
flow, in particular perfusion pressure, blood flow
velocity and shear stress in the coronary arteries,
results in the release of vasodilators (NO) and the
release of angiogenesis factors (VEGF). Basically,
the method is used to treat angina pectoris, coronary
heart disease.
This paper describes a method and apparatus for
the treatment of peripheral arterial diseases using
cardiosynchronized pneumatic compression, which
are a development of the previously proposed
methods.
58
Sudarev, A. and Korotich, E.
The Method and Apparatus for Peripheral Arterial Disease Treatment.
DOI: 10.5220/0010828100003123
In Proceedings of the 15th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2022) - Volume 1: BIODEVICES, pages 58-65
ISBN: 978-989-758-552-4; ISSN: 2184-4305
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
2 METHOD AND EQUIPMENT
The authors proposed a method of treatment for
PAD - cardiosynchronized sequential antegrade
pneumocompression (CSAP) (Sudarev A.M.,
Sudarev A.M., Korotich E.V.).
In this method, an effective formation of an
antegrade (i.e. towards the distal extremities) wave
is achieved by periodic compression of each affected
limb separately in two zones - proximal and distal.
Compression pulses in the distal zone are delivered
after pulses in the proximal zone with a controlled
delay.
This pressure wave should enhance blood flow
in the distal areas, increases the hydrostatic pressure
and shear stress in the vessels in the areas below the
affected zones, and increases tissue perfusion.
Arterioles and capillaries were chosen as the main
targets of exposure.
To obtain the desired effect, a pressure is created
in the cuffs that exceeds the level of systolic blood
pressure, which leads to the collapse of the arteries
and an intensive redistribution of blood to the
surrounding regions (Bonetti P.O. et al). A pressure
wave arises, propagating in both directions from the
point of occlusion. Compression of the second cuff
located distal to the first leads to an increase in the
pressure wave. In this case, the compression of the
first cuff is a "gate" for the blood pushed out from
the sections of the vessels located under the distal
cuff. The formation of pressure waves is
schematically shown in
Figure 1. This scheme of
action is similar to a peristaltic pump.
Figure 1: Impact mechanism.
For comparison, we present the schemes of
exposure for EECP and CSAP (
Figure 2, Figure 3).
Figure 2: EECP diagram.
Figure 3: CSAP diagram.
In contrast to sequential rhythmic pneumatic
compression, the external pressure slew rate value is
fundamentally important, because the change in
microcirculation in the distal regions, especially in
the terminal arteries, arterioles and capillaries,
depends on the compression slew rate in the
proximal region. As shown in (Conti C.R et al,
Bonetti P.O. et al), with a decrease in the pressure
pulse leading edge duration, the maximum attainable
pressure in the outer regions increases. Accordingly,
an increase in arterial pressure leads to an increase in
capillary blood flow. With a slow slew rate, the
pressure wave outside the compression zone is
shunted by the collaterals and does not reach its
maximum possible magnitude.
It was proposed to synchronize the compression
pulses with the cardiac cycle in order to ensure the
optimal superposition of the native pulse wave with
the wave created by pneumatic compression for the
most effective increase in perfusion pressure, and,
accordingly, blood flow in the distal regions.
As will be shown below, this synchronization
may be beneficial for two reasons: it increases the
blood flow in the extremities, and it increases the
blood flow in the myocardium with a simultaneous
decrease in the systolic work. At EECP usage only
the second goal is usually achieved.
The Method and Apparatus for Peripheral Arterial Disease Treatment
59
For the maximum amplification of the wave
propagating in the antegrade direction, the moment
of the beginning of limb compression was proposed
to be synchronized with the propagation of the
natural pulse wave maximum through the
compression zone. In this case, the superposition of
these two waves is maximum. This moment
corresponds to the ejection phase at the orifice of the
aorta plus a delay in the propagation of the pulse
wave from the orifice of the aorta to the site of cuff
application. The delay of the impulse in the distal
cuff relative to the proximal one should be of the
order of the time of propagation of the pulse wave
between the cuffs.
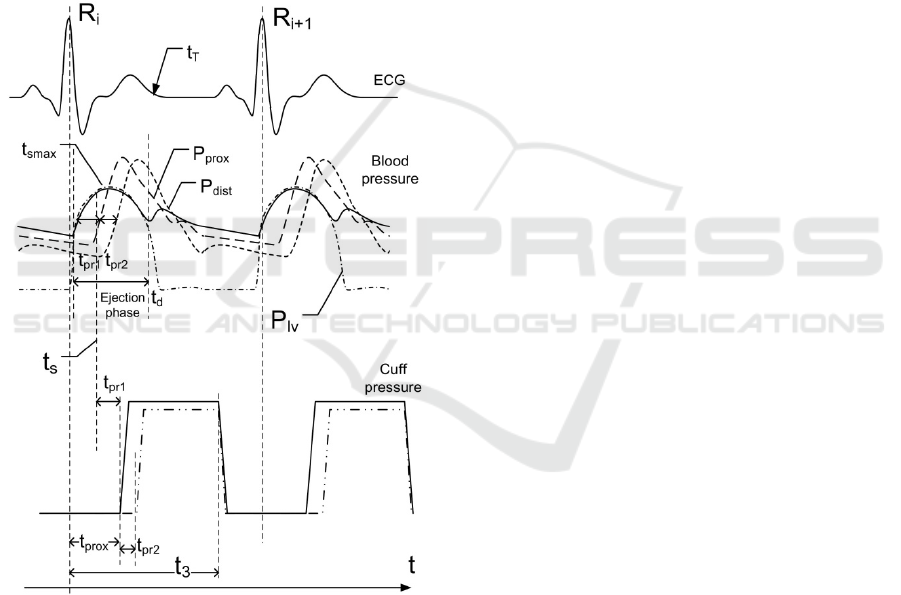
The timing diagram of the exposure is shown in
the
Figure 4.
Figure 4: CSAP timing diagram.
Therefore, to maximize the antegrade wave, the
time of the onset of the pulse in the proximal cuff is
estimated as follows: t
prox
= t
s
+ t
pr1
, where t
s
is the
moment in the interval from the beginning of the
ejection phase to the moment of the systolic
maximum pressure t
smax
at the aortic orifice, and t
pr1
is the time of propagation of the pulse wave from the
aortic orifice to the site of the proximal cuff. More
accurate determination of t
prox
could be made
experimentally.
On average, t
smax
(systolic maximum) is
separated from the R-peak of the ECG by a time of
the order of 0.15 ÷ 0.2 sec.
In this case, t
pr1
= L
1
/ v, where v is the speed of
the pulse wave in large arteries (4–7 m/sec (Caro
C.G. et al)), and L
1
is the distance from the aortic
orifice to the site of the proximal cuff. When the cuff
is applied to the hip, t
pr1
is about 0.05 ÷ 0.1 sec. This
gives t
prox
(delay in the onset of compression in the
hip cuff relative to the R-peak of the ECG) of the
order of 0.2 - 0.3 sec.
The delay between pressure pulses in the
proximal and distal cuffs is t
pr2
= L
2
/ v, where L
2
is
the distance between the cuffs, which for t
pr2
gives
about 0.03 ÷ 0.06 sec.
When the vessels are compressed by the
proximal cuff, a retrograde pressure wave is also
formed, propagating towards the aorta. To increase
coronary blood flow in this case (similar to the case
of external counterpulsation) it is necessary that it
reaches the aortic orifice during diastole. Thus, the
lower limit for the beginning of the pressure in the
proximal cuff is as follows: t
prox
≥ t
d
-t
pr1
, where t
d
is
the end of the ejection phase (the aortic valve
closure time is about 0.3 sec, approximately
corresponding to the end of the T-peak of the ECG
(Caro C. G. et al)), which gives the limit for t
prox
-
not less than 0.15 ÷ 0.25 sec.
The inflation of the cuffs should be carried out
simultaneously before the onset of mechanical
systole in order to ensure a decrease in the
mechanical work of the heart, similar to the method
of EECP (Conti C.R et al).
The described method of exposure was
implemented on the basis of the system for external
counterpulsation CARDIOPULSAR™ (CONSTEL
LLC, Russia) (www.constel.ru).
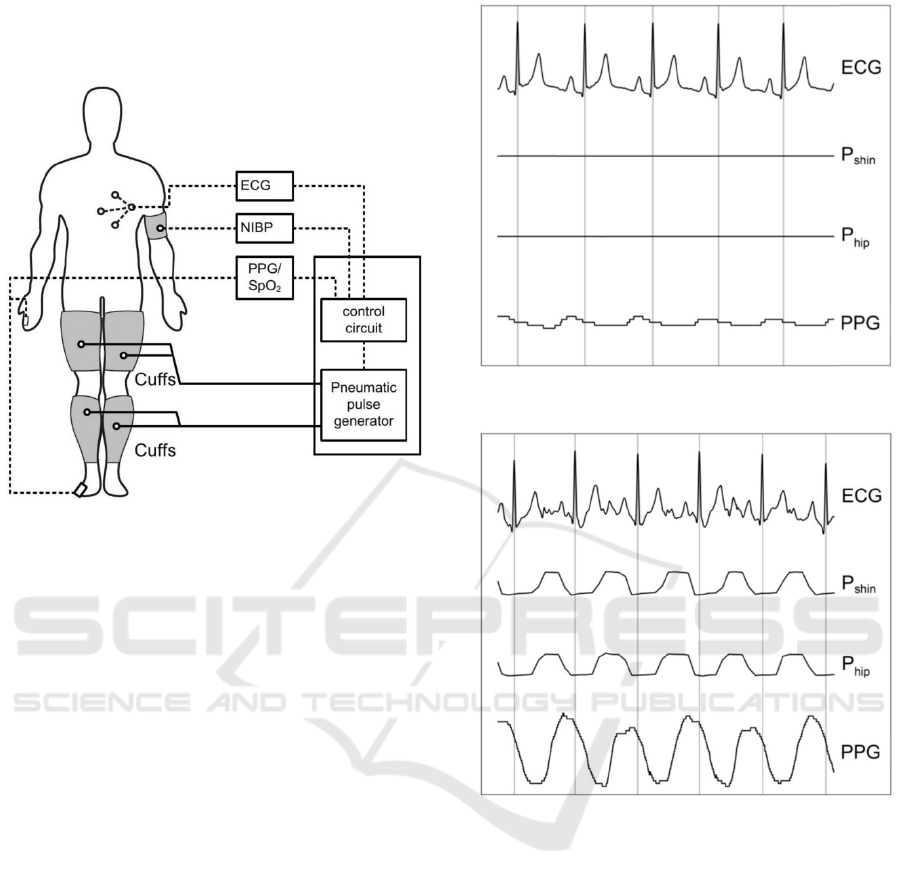
The general scheme of the device in the
antegrade pneumocompression mode is shown in
Figure 5. The hip and shin cuffs are used as
proximal and distal cuffs, respectively. To
synchronize the pressure pulses in the cuffs, an
electrocardiogram (ECG) signal was used. Pressure
pulses in the cuffs, are given taking into account the
delay of the incoming pulse wave in relation to the
R-peaks of the ECG. To create the necessary time
diagram of the compression effect on the lower
extremities the software of the CARDIOPULSAR™
system was modified. A photoplethysmogram sensor
placed on the toe was used to monitor changes in
blood flow. This sensor can also be used to optimize
the exposure timing.
BIODEVICES 2022 - 15th International Conference on Biomedical Electronics and Devices
60
An experimental study of the physiological
effect of our proposed new method of
pneumocompression (CSAP) was carried out.
Figure 5: Device diagram.
3 EXPERIMENTAL STUDY AND
RESULTS
To study the effect of the cardiosynchronized
compression on the circulatory system of the
extremities in practically healthy people and patients
with PAD an experimental study was carried out to
assess the change in blood flow in a toe.
The experimental studies involved volunteers: 4
apparently healthy adult men aged 22 to 50 years
and 10 patients with atherosclerosis of the lower
extremities, chronic vascular insufficiency of groups
2A and 2B aged 45 to 65 years.
Each episode included a standard 60 minute
session.
The graphs (Figure 6 and Figure 7) show typical
physiological signals without compression impact
(Figure 6) and with impact (Figure 7): ECG signal,
cuff pressure plots (hip and shin) and a
photoplethysmograph signal (PPG) reflecting the
pulse blood filling in the toe.
The difference between ECG signals (Figure 6
and Figure 7) is due to mechanical artifacts during
periodic compression.
It can be seen that during the application of the
compression, an increase in the pulse wave occurs.
The characteristic increase in the PPG amplitude
compared to the initial level is 2 to 4 times.
Figure 6: ECG, cuff pressure and PPG before exposure.
Figure 7: ECG, cuff pressure and PPG during exposure.
We studied the influence of the amplitude-time
parameters of pneumatic pulses on the
hemodynamic effects. Particularly the dependences
of the increase in blood flow in the distal part of the
limb (PPG amplitude on the toe) vs the amplitude of
the compression pulses and their delay relative to the
R-peak of the ECG, were investigated.
The dependence of the PPG amplitude on
compression pressure was measured by a sequential
increase in the amplitude of the compression pulses
with a step of 10 mm Hg approximately every 20
sec. Typical dependences (on 4 subjects coded as
S1, S2, S3, S4) in an experiments with a normal
level of systolic pressure (<140 mm Hg) of the PPG
amplitude vs compression pressure are shown on
Figure 8 (solid lines show the interpolation of trends
by fourth-order polynomials).
The Method and Apparatus for Peripheral Arterial Disease Treatment
61
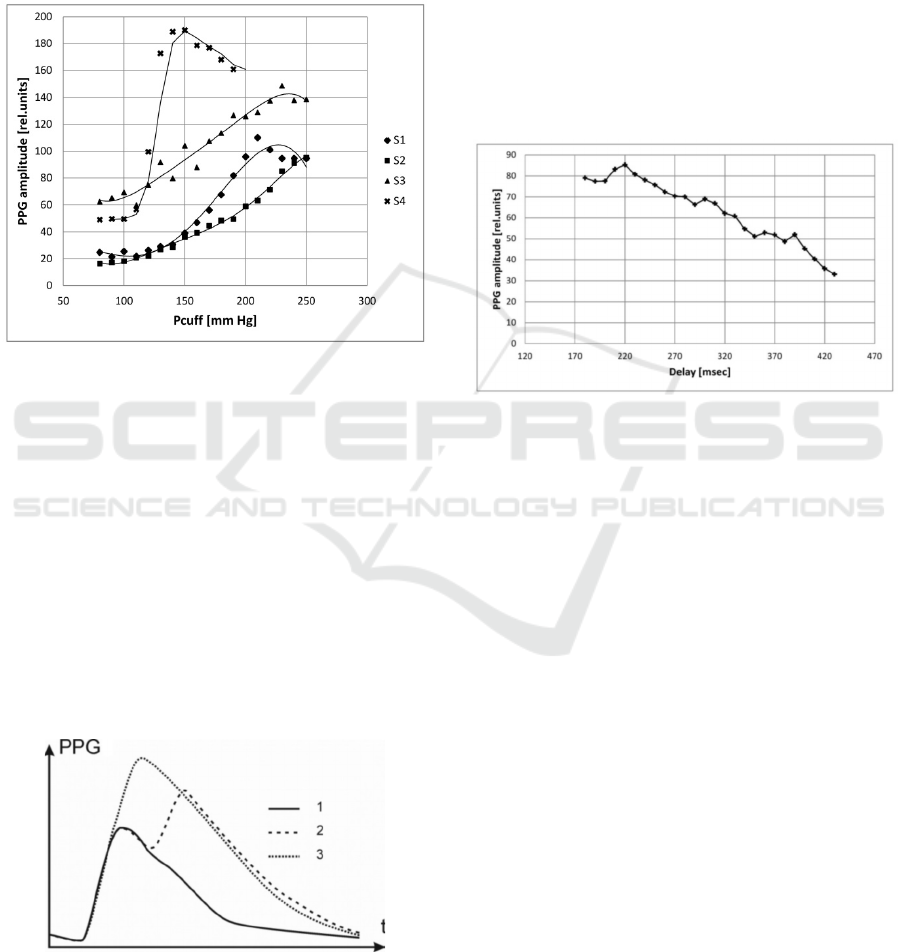
It can be seen that the dependences have a
characteristic S-shape. The beginning of the growth
of the PPG amplitude begins at compression
pressures of 100-120 mm Hg. The maximum values
are reached at pressures of 150-250 mm Hg, which
corresponds to systolic blood pressure. These results
indicate that the maximum effect is achieved with
collapse of the arteries under the cuffs.
Figure 8: PPG amplitude on the toe vs cuffs pressure.
The amplitude of pneumatic pulses required to
maximize blood flow in the distal regions are
slightly more than systolic blood pressure. It could
be explained by the fact that the actual mechanical
stress of the underlying tissues is slightly less than
the pressure in the inflatable chambers. The
difference therefore depends on the type of
compression cuffs (their geometric and design
features).
The dependence of the shape and the resulting
amplitude of the pulse wave on the delay in the
onset of the pressure pulse in the proximal cuff was
studied. The characteristic shape of the PPG signal
at different delays looks is shown in Figure 9.
Figure 9: 1 - No action, 2 - long delay, 3 - optimal delay.
The dependence of the PPG amplitude on the toe
on the delay between the R-peak of the ECG and the
onset of compression in the femoral cuff was
investigated experimentally. A typical dependence
of the averaged PPG amplitude over approximately
20 cardiac cycles is shown in Figure 10. On the
graph, the ordinate shows the delay between the R-
peak and the moment when the pressure in the cuff
has reached the amplitude value. In this case, the
delay between the onset of impulses in the hip and
shin cuffs was constant (40 msec). It should be noted
that the reported values of the delay may have an
error of the order associated with the inaccuracy of
the formation of pressure pulses (10–20 msec)
relative to the R-peak, as well as with the duration of
the pulse front (approximately 70–90 msec).
Figure 10: Dependence of the PPG amplitude on the delay
between the R-peak and the moment of reaching the
nominal pressure in the pulse in the hip cuff.
The graph repeats the characteristic shape of
PPG (maximum (plateau) at low values and a
smooth decline with increasing delay). This
dependence characterizes the superposition of two
waves in the distal regions: a natural pulse wave and
a wave caused by compression (similar to the effects
observed with external counterpulsation).
As a result, the shape and amplitude of the
photoplethysmogram in the distal parts of the limb
may be used as a feedback signal for more accurate
adjustment of the exposure time diagram (Sudarev
A.M., Korotich E.V.), since the time of occurrence
and the degree of actual compression of the tissues
of the extremities by the cuffs depends on often
uncontrollable factors: the delay in the measuring
and acting tract, the design and degree of the initial
tightening of the compression cuffs, the speed of
propagation of the pulse wave, etc.
To achieve the maximum effect it is necessary to
adjust the delay and the magnitude of the pneumatic
impulse pressure achieving the maximum PPG
amplitude and the approach of the moment of the
maximum of the amplified blood flow wave to the
systolic maximum of the natural wave. It should be
BIODEVICES 2022 - 15th International Conference on Biomedical Electronics and Devices
62

noted that the decrease in latency should be limited,
since the resulting retrograde wave should reach the
aortic orifice in the diastolic phase. An excess value
of the compression pressure leads to unwanted
trauma to the underlying tissues without leading to
an effect increase. This is evidenced by the
saturation of the dependence of the increase in blood
flow when the compression pressure is exceeded by
more than 50-70 mm Hg above the systolic pressure
levels (Figure 8).
To compare the hemodynamic effect in the distal
parts of the limb in the CSAP and EECP modes,
experiments were carried out in which the change in
the PPG amplitude on the toe in these modes relative
to the background level was compared. The gain was
measured as K
ampl
= PPG
exp
/ PPG
back
, where PPG
exp
is the amplitude of PPG during exposure, and
PPG
back
is the amplitude of PPG without exposure.
In healthy volunteers (5 test subjects, 2 experiments
carried out at different times), K
ampl
in the CSAP
mode was 1.8 ± 0.3 times higher than in the EECP
mode.
Subsequently data on the greater efficiency of
enhancing blood flow in the distal regions in the
CSAP mode compared to EECP were repeatedly
confirmed (in more than 100 patients with PAD) in
clinical studies (Atkov O. U. et al).
It is known that the distal parts of patients with
PAD are often colder due to circulatory
insufficiency. To investigate changes in limb
circulation in two patients with PAD, a study was
carried out using a thermal imager (IRTIS-2000,
Russia).
The surface temperature of the skin, especially
the limbs, measured by the thermal imager varies
greatly depending on many factors. The
experimental conditions (external temperature and
long-term adaptation to the lying position) were
selected in such a way as to minimize the natural
temperature drift as much as possible.
The results of a typical experiment are shown in
Figure 11and Figure 12.
The temperature of the toes increases markedly
10-30 minutes after the start of the procedure (up to
1-2 ° C). In addition, preliminary data show that the
temperature of the feet increases after a course of
procedures. An increase in foot temperature
indicates an integral increase in blood circulation.
In the initial period of the study of the
effectiveness of the treatment, a series of procedures
was carried out in volunteer patients with PAD
(diagnosis: atherosclerosis of the lower extremities,
chronic vascular insufficiency, stages 2A and 2B by
Fountaine), which made it possible to assess the
change in the course of the disease and draw a
conclusion about the clinical effect. The studies
involved 10 patients. Each patient underwent 12 to
15 procedures, 60 minutes each.
Figure 11: Thermal image before exposure.
Figure 12: Thermal image (30 min after start of exposure).
The Method and Apparatus for Peripheral Arterial Disease Treatment
63

All patients showed an increase in exercise
tolerance (6-minute walk test until the onset of
discomfort and pain in the shin muscles). The
increase in distance was from 22 to 100% after the
first two procedures.
The measurements of the ankle-brachial index
(ABI) were also carried out, calculated as the ratio
of arterial systolic pressure in the distal parts of the
legs to systolic pressure in the brachial arteries.
After a cycle of procedures in each of the patients,
the index increased by 0.1 ± 0.05 with the initial
values from 0.7 to 0.8.
In all patients with disease stages 2A and 2B,
after the first procedure, subjective improvement
was noted: discomfort in the limb, a feeling of
coldness, especially in the distal parts, a feeling of
cold in the legs, the need to keep the distal part of
the limb warm during sleep, etc.
After receiving the first positive results, a
multiclinic study of the effectiveness of the proposed
therapeutic method was carried out on a large group
of patients with multifocal atherosclerosis (Atkov O.
U. et al). This study showed that the use of the
method and the CARDIOPULSAR device leads to
an increase of pain-free walking distance, an
increase of ankle-brachial pressure index (ABPI),
and an improvement of microcirculation. The
improvement of life quality estimated by DASI
Activity Index and Edinburgh Claudication
Questionnaire (ECQ) was also shown.
4 CONCLUSIONS
The method and device of pneumatic compression
effect on blood circulation of the extremities for the
treatment of PAD achieving an effective increase in
blood flow in the distal regions have been developed.
The primary hemodynamic effects of exposure
and the dependence of an increase of blood flow in
the distal regions on the amplitude-time
characteristics of pneumatic pulses were studied.
The results of clinical application of the method
on volunteer patients suffering from PAD
(obliterating atherosclerosis, endarteritis, diabetic
angiopathy) have been obtained, which indicates its
promising potential.
ACKNOWLEDGEMENTS
We would like to thank the following people who
have helped us undertake this research:
Prof. Gennady G. Amosov (R.I.P.) for inspiring us
initial ideas and cooperation,
The CONSTEL LLC staff that helped us in any
aspects and especially Oleg Uss and Lev Mershin
for help in preparation of the text.
REFERENCES
Atkov O. U., Zudin A. M., Shugushev Z. H ., Orlova M.
A., Sudarev A. M., Korotich E. V., Maximkin D . A.,
Patrikeev A. V. (2015) Short-term results of
cardiosynchronized consequential antegrade
pneumocompression in patients with multifocal
atherosclerosis Rossijskij kardiologicheskij zhurnal
(Russian Journal of Cardiology), 3 (119): 82–88
Benjamin et al. (1978) Apparatus for promoting blood
circulation. Pat. US 4077402
Bonetti P.O., Holmes D.R., Lerman A., Barsness G.W.
(2003) Enhanced external counterpulsation for
ischemic heart disease - What's behind the curtain?
Journal of the American College of Cardiology.; 41:
11: 1918-1925
Caro, C. G., Pedley, T. J., Schroter, R. C. and Seed, W. A.
(1978) The Mechanics of the Circulation, Oxford
University Press. (527 pp.)
Conti C.R., (1999) EECP-Enhanced External
Counterpulsation, Journal of the American College of
Cardiology.; 33: 7: 1841-1842
Delis K.T., Knaggs A.L. (2005) Duration and amplitude
decay of acute arterial leg inflow enhancement with
intermittent pneumatic leg compression: an insight
into the implicated physiologic mechanisms. J Vasc
Surg.; 42(4): 717-25.
Dillon R.S. (1997) Fifteen years of experience in treating
2,177 episodes of foot and leg lesions with the
circulator boot. Angiology.; 48: 17-34
Dillon R.S. (1996) Method for promoting circulation of
blood. Pat US 5514079
Dormandy, J & Mahir, M & Ascady, G & Balsano, F & de
Leeuw, Peter & Blombery, Peter & Bousser, M &
Clément, Daboné & Coffman, J & Deutshinoff, A.
(1989). Fate of the patient with chronic leg ischaemia.
A review article. The Journal of cardiovascular
surgery. 30. 50-7
Fowkes, F.G.R. & Housley, E & Cawood, E.H.H. &
Macintyre, Colin & Ruckley, C.V. & Prescott, Robin.
(1991). Edinburgh Artery Study: Prevalence of
Asymptomatic and Symptomatic Peripheral Arterial
Disease in the General Population. International
journal of epidemiology. 20. 384-92.
Lipnitsky E.M., Amosov G.G., Morozov K.M., Zateryukin
A.B., Platonov A.Yu., Vaidya A. (2007) Rhythmic
pneumocompression for treatment of patients with
chronic obliterating diseases of the lower-limb arteries
Angiologiya i sosudistaya hirurgiya (Angiology and
vascular surgery). 13: 3: 22-26 (in Russ.)
Sudarev A.M. (2013) Treatment for chronic obliterating
diseases of lower limb arteries. Angiologiya i
BIODEVICES 2022 - 15th International Conference on Biomedical Electronics and Devices
64

sosudistaya hirurgiya (Angiology and vascular
surgery) 19, 1 . 26 -32 (in Russ.)
Sudarev A.M., Borodyanskaya E.S., D'yachenko A.I.
(2010) Modeling of external counterpulsation
gemodynamic effects by means of electrical analogs.
III Evrazijskij kongress po medicinskoj fizike i
inzhenerii "Medicinskaya fizika - 2010"; 4: 106-108
(in Russ.)
Sudarev A.M., Korotich E.V. (2016) Method and devices
providing impact on cardiovascular system. Pat. US
US2013102939
The Method and Apparatus for Peripheral Arterial Disease Treatment
65
