
Health-CAT: Development of a Mobile Robot for Assisting Caregivers
William K. Juel
a
, Frederik Haarslev
b
and Leon Bodenhagen
c
SDU Robotics, University of Southern Denmark, Campusvej 55, Odense C, Denmark
Keywords:
Healthcare Robotics, Human-robot Interaction, Participation.
Abstract:
The demographic change is expected to challenge the healthcare sector which in many countries is already
struggling today leading to, e.g., a shortage of staff. Since robot technology is playing a minor role in health-
care today, robotics is considered to be one mean to mitigate some of the challenges related to the demographic
changes. This paper discusses hurdles for introducing robotics solutions in healthcare and describes the identi-
fication of a use case as well as the development of a robot prototype. End users have been involved throughout
an iterative development process leading to a prototype that has been tested during normal operations.
1 INTRODUCTION
The demographic change is challenging many health-
care systems. Not only is the share of citizens in the
working age declining but also the demand for health-
care services is increasing since the number of el-
derly citizens is growing and this population group
has a higher prevalence for comorbidities. Already
today a shortage of staff can be observed in the care-
giving domain (Drennan and Ross, 2019) which only
can be expected to worsen given both the general de-
mographic development and, recently, the increase
of the turnover intentions amongst nurses during the
COVID-19 pandemic (Falatah, 2021).
Lately substantial progress has been achieved in
the domain of robot technology in general, includ-
ing related areas such as computer vision or artifi-
cial intelligence. However, unlike the industrial do-
main, robots are currently only playing a minor role in
healthcare, apart from niche applications such as sur-
gical robotics or pilot cases. Therefore robotics can
be considered to present a not yet utilized potential
mean for at least partially mitigating the demographic
challenge (Bodenhagen et al., 2019).
The Health-CAT project
1
was initiated prior to the
pandemic and focuses on identifying how robot tech-
nology that is largely already available can be ex-
ploited to support care givers and develops and tests
a prototype of such a robot. Throughout the project
a
https://orcid.org/0000-0001-5046-8558
b
https://orcid.org/0000-0003-2882-0142
c
https://orcid.org/0000-0002-8083-0770
1
Health-Care Assisting Technology, https://healthcat.eu
there was a focus on the involvement of the end-users
for identifying a use case that remains relevant in the
light of the demographic change and generating an
understanding of how a robot should be integrated
into existing workflows.
2 BACKGROUND
Given the shortage of staff and an increasing demand
for services, healthcare could be considered to be able
to benefit from the implementation of robotic solu-
tions. However, while the expenditures for health-
care in OECD countries amount to around 10 % of
the GDP (OECD, 2014), it only plays a minor role
in the application of robotics. The majority of ap-
plications outside the industrial domain are related
to logistics where 10 times as many installations are
reported compared to medical robotics (International
Federation of Robotics, 2020).
A large variety of robots for applications within
healthcare can be found in the literature (see, e.g.,
(Holland et al., 2021)), ranging from topics such
as hygiene which got an increased focus during the
covid-19 pandemic where, e.g., mobile robots have
been equipped with UV-light emitting lamps for san-
itizing surfaces, to handling of samples or social
robots. While the development of robotic solutions
for less structured environments can be challenging,
mobile robots are for instance able to operate safely
and largely autonomously in environments shared
with humans which suggests that solutions for mo-
bile robots should be feasible to achieve. However,
Juel, W., Haarslev, F. and Bodenhagen, L.
Health-CAT: Development of a Mobile Robot for Assisting Caregivers.
DOI: 10.5220/0010840800003124
In Proceedings of the 17th International Joint Conference on Computer Vision, Imaging and Computer Graphics Theory and Applications (VISIGRAPP 2022) - Volume 2: HUCAPP, pages
171-178
ISBN: 978-989-758-555-5; ISSN: 2184-4321
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All r ights reserved
171
Figure 1: Steps taken to come from focus areas to use case
formulation.
besides technical challenges, also various additional
challenges such as a negative reputation of robots,
workflows being altered, the fear of jobs to be taken
over by robots or unclear liability are considered im-
portant to be addressed (Cresswell et al., 2018; Radic
et al., 2019). In addition, ethical aspects related to the
consequences, such as the potential reduction of hu-
man contact or the handling of privacy, of introducing
robots are considered important for achieving accept-
ability (Stahl and Coeckelbergh, 2016).
The Health-CAT project focuses on the devel-
opment of a healthcare robot involving end users
throughout the process to develop a use case that is
both feasible but also relevant and where the integra-
tion of the robot into existing workflows has been a
integrated part of the design process. Ethical chal-
lenges have been taken into account during the selec-
tion of the use case to minimize the risk for a later
implementation of the robot to be inhibited by ethical
aspects and potential negative publicity.
In the following the overall approach is outlined
(section 3) followed by a needs analysis (section 4)
that culminates in the formulation of a specific use
case and a test of solution for this use case. Details of
the technical development are provided in section 5.
3 METHOD
When developing and implementing new technology,
it is essential to have an understanding of the end
users and the context of the developed solution. It en-
sures that the solution will fulfil an actual need rather
than, potentially driven by technology, formulating
new applications for existing technologies. In addi-
tion, it ensures a preparation of possible challenges of
the solution - for instance physical limitations, differ-
ent levels of competencies among users or unwilling-
ness to adopt new technology amongst others. Fur-
thermore, involving end users of the technology at an
early stage often pays off in the implementation pro-
cess, because the users get a sense of ownership to the
final solution.
Health-CAT focuses on the general needs of the
healthcare sector and its users. We involved the users
(staff at German and Danish hospitals and care cen-
ters) during every step in the development process to
determine actual requirements for a robot prototype.
The feedback of the users was utilized in the subse-
quent steps in the development process. Thereby we
ensure to always meet the needs of the users. In the
following (section 4 the needs analysis, starting with
desk research and progressing via multiple mock-ups
to the final prototype, which was performed in the
Health-CAT project will be described.
4 NEEDS ANALYSIS
The overarching goal in the Health-CAT project is to
investigate use cases in the healthcare sector where
robot technology can create value and help mitigat-
ing the challenges related to the demographic change.
We want to ensure that the quality of care does not
decrease in our future healthcare system that is chal-
lenged by to the expected issues arising from the soci-
etal challenges described in section 1. A needs analy-
sis was conducted based on broad involvement of pa-
tients and healthcare employees. The analysis con-
sist of desk research, ethnographic observations, in-
terviews and focus-group interviews. Initially desk
research was conducted to find societal challenges
that later was further investigated through observa-
tions and interviews at different healthcare institu-
tions in Denmark and Germany. In total 20 inter-
views with patients and 62 interviews with employees
at healthcare institutions ranging from nurses, care-
givers, doctors, service- and kitchen staff was con-
ducted. The needs analyses attempts to:
• Identify focus areas where healthcare profession-
als have a need to be relieved in their daily work.
• Evaluate, how these workflows can be supported
by robot technology
• Map the barriers and challenges with implemen-
tation of robot technology.
Finally the needs analysis points towards several
scenarios where robot technology could play a role.
In order to conduct a qualified identification of
needs, it was crucial to gather input from many differ-
ent types of employees in the healthcare sector so that
the needs analysis will represent needs across differ-
ent parts of the healthcare sector. The first step in the
HUCAPP 2022 - 6th International Conference on Human Computer Interaction Theory and Applications
172

needs analysis was to identify existing potential prob-
lems within the healthcare sector in our case in Danish
hospitals and German nursing homes, see figure 1 for
an overview of our process. The context is analyzed
at three levels macro, meso and micro. The macro
and meso levels was studied by conducting literature
search and expert interviews with e.g. union repre-
sentatives. The output of researching these two levels
was a list of 10 potential focus areas within Health-
care that could potentially be supported by robot tech-
nology:
1. Hygiene: poor cleaning
2. Poor oral hygiene: pneumonia
3. Malnutrition and lack of follow-up
4. Overweight and obesity
5. Transporting equipment and patients
6. Inappropriate medication
7. Rehabilitation
8. Documentation
9. Cultural diversity
10. Measuring health parameters
These areas are then qualified by the project part-
ners as well as relevant hospital employees. After
conducting interviews, it was possible to map com-
mon focus areas of potential interest, which was then
agreed on by project partners, relevant stakeholders
and users. This final qualification was conducted in
a workshop, and resulted in a list where 6 of the ini-
tial focus areas got discarded and 4 was kept, these 4
focus areas was further discussed and detailed into 7
sub areas, see figure 2.
With these relevant focus areas identified, we fur-
ther wanted to validate them by interacting with rele-
vant employees and observing the work flow within
the potential focus areas at both hospitals and care
centers.
4.1 Field Work
A field work protocol including an interview guide
and an observation guide was created. The protocol
defines who to interact with, how many, where, and
how to document the interactions. The field work
was conducted in a Danish hospital and in German
care centers, we identified specific workflows, user
needs, potentials and challenges, within the focus ar-
eas of interest. An observer’s ability to observe can
be influenced on whether the observer is in advance
familiar with the observed workflows or not. The
research team therefore included both a Healthcare
professional and an engineer with a technical back-
ground conducting the field work. The field work
process lasted 1.5 month in Germany and 2.5 month
in Denmark with a total of 63 people from relevant
roles being observed and interviewed. The intention
was to interview both employees and patients in hos-
pitals, as well as employees and residents in nursing
homes. However, several of the patients in the geri-
atric department at the hospital suffer from cognitive
impairment, which made it challenging to interview
the patients. As a consequence only two patients was
interviewed, see table 1 for more information about
the field work.
The data received from the field work was further
analyzed at a workshop and 5 focus areas was further
detailed in the form of concrete robotic use cases:
• Cleaning of wheelchairs, toilet chairs, beds, night-
stands
• Transportation of food
• Transportation of small equipment
• Transportation of large equipment
• Hand hygiene of patients and employees
4.2 Use Case Analysis
In the following the focus areas will be further intro-
duced and potential use cases are outlined. In the con-
ceptualization of the use cases ethical challenges in
regard to introduction of robot technology was highly
important and likewise was technical challenges, the
solutions had to be technically feasible with today’s
technology while at the same time not cause any kind
of ”harm” to the employees. This could be altering
their workflow excessively or creating technology that
could end up being a liability.
Area: Cleaning of Wheelchairs, Toilet Chairs,
Beds or Nightstands
During observations and interviews, it was clear that
the health carers do not consider cleaning as their pri-
mary task. Furthermore, there is not allocated any
space for cleaning and the consequence is cleaning
of equipment takes place in the hallways or in bath-
rooms. Another consequence is bad work postures,
as the employees do not have any tools available for
easing the cleaning process. Therefore, the employ-
ees have to reach all parts of the equipment manually,
including difficult accessible parts like wheels or the
bottom of a nightstand and we observed that it was not
cleaned properly due to several of the above issues.
Potential Use Case: Automated Washing Machine
Transport to Automated Washing Machine: The em-
ployees use different types of equipment as part of
nursing tasks. Before or during use, the employee
Health-CAT: Development of a Mobile Robot for Assisting Caregivers
173
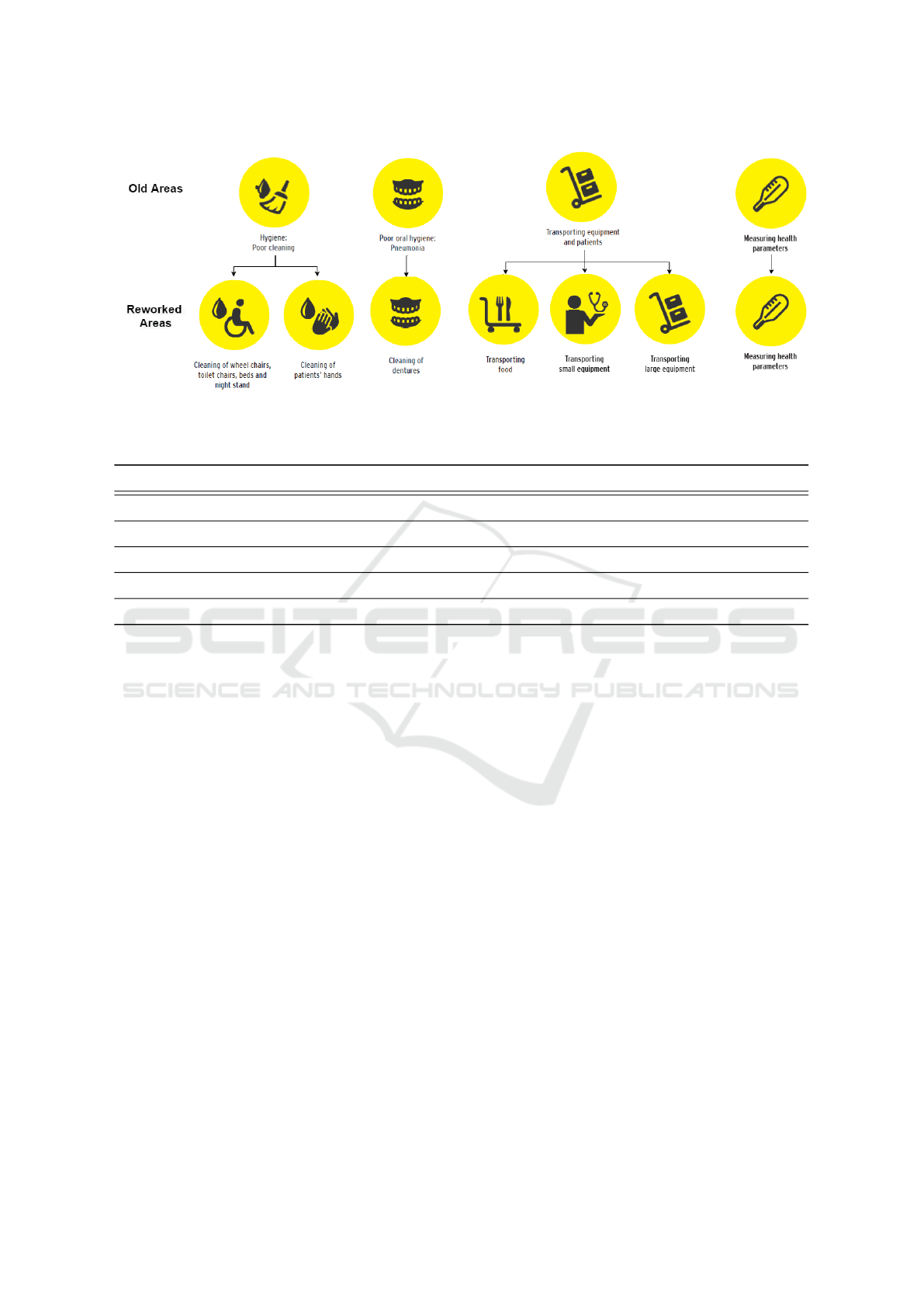
Figure 2: The 10 initial focus areas have been filtered to 4 (top row), excluding those that have been considered to be infeasible,
and detailed further. This leads to 7 reworked focus areas (bottom row).
Table 1: Field work information.
Country Germany Denmark
Location of Observation Tabea, nursing home and UKSH, hospital SHS Aabenraa, hospital
Ward Orthopedics and Trauma Surgery Geriatric
# of employee observations 14 28
# of employee interviews 14 27
# of interviews with patients or residents 19 2
calls a robot to place itself right outside the pa-
tient’s room. When the employee is done using the
equipment, the employee places the equipment on
the robot, and the robot transports the equipment to
the automated washing machine. After cleaning, a
robot transports the equipment back to the designated
equipment space.
The equipment cleaning: The robot automatically
places the equipment on a conveyor belt. The belt will
transport the equipment into the automated washing
machine, where it is automatically cleaned and dried.
Area: Transportation of Food
Transportation of food is a time consuming task due
to registration of intake, ordering and serving of food
and it requires a lot of walking. In the morning the
kitchen staff have to prepare and transport food to
all wards at the same time which creates a crowded
kitchen area. At noon and in the evening the food is
transported to the ward by the kitchen staff and the
health carers helps the patients eat. The health carers
and the kitchen staff do not coordinate their tasks so
the patients’ meals is sometimes stranded in the hall-
way for a while before the health carers have time to
serve food to patients. Furthermore, the registration
of patients’ food intake is often a challenging tasks
since it is time consuming and meals are brought to
the patient by one employee and picked up by another.
Use Case: Food Transport and Registration
Transportation of Food: Health carers order meals
and kitchen staff loads a robot (with a combined
heating- and cooling cabinet) with trays of meals for
a specific ward. The robot registers food for the each
patient or resident and drives to the specific ward. The
health carers pick up and serve trays for patients or
residents one by one.
Registration of food: When the patients or residents
are finished eating, the health carers pick up the trays
and load the robot. The robot registers food intake
(calories) for each patient or resident and uploads data
automatically (e.g. in Cosmic or Dankost) and returns
to the kitchen.
Area: Transportation of Small Equipment
As part of care-giving, the health carers need small
equipment, such as venflons, bandages etc. The
health carers have to leave the patients, walk to the
storage, pick up small equipment, walk back to the
patient and continue their original task. If equipment
is damaged the procedure is repeated. The health car-
ers cannot bring spare equipment, due to a policy to
minimize waste. Collection of small equipment is an
issue since it is a time consuming task that requires
walking up to 10 km a day. Patients and residents of-
ten experience the situation as both time consuming
and confusing since the staff interrupts their routine.
HUCAPP 2022 - 6th International Conference on Human Computer Interaction Theory and Applications
174

If small equipment has been brought along to a pa-
tient room without being used, it has to be discarded
due to risk of infection. One specific observation that
illuminates this issue was patch being fetched which
took up to 5 minutes.
Potential Use Case: Mobile Dispenser
Each ward has a number of robots with a dispenser
mounted that is filled with small equipment, specific
to the ward’s requests. The refilling of all robots is
done by e.g. a service assistant in the basement. Af-
ter refilling, the robots drive to the ward and wait in
allocated spaces in the hallway. When equipment is
needed, the health carers visit the robot or call it to the
room via. a call system installed on the ward. When
the robot is low on inventory, it automatically calls a
another robot to replace it. The empty robot drives to
the storage, where it will be refilled and cleaned by a
service assistant.
Area: Transportation of Large Equipment
When equipment is needed for a nursing task, the
health carers start searching in hallways before look-
ing in the allocated space since equipment is often not
positioned at the allocated space. In German nurs-
ing homes, we observed that health carers interrupt
their colleagues just to locate equipment. Once the
equipment is located, and if not in use, the health car-
ers transport the equipment manually. Due to lack of
time, equipment is often left without proper cleaning,
which mean the next person have to clean it before
using it.
Potential Use Case: Equipment Caddy
When large equipment is needed, the healthcarers call
a robot via. a tablet, to bring required item to the de-
sired area. The healthcarers can also locate equip-
ment on the tablet, and pick it up and manually. If
equipment is already in use, it will display a waiting
list. After use, equipment is loaded on the robot. The
robot transports the equipment to the next user or to
allocated free space. Thereby healthcarers can con-
tinue there routines and be more efficient.
Area: Hand Hygiene of Patients and Employees
As part of the morning routine in hospitals in both
Germany and Denmark, the patients get a cloth or
a wet tissue. It is up to the patients to assess what
to clean. From our observations, most patients for-
get to clean their hands thoroughly. During the day
there was little or no focus on cleaning of patient’s
hands, neither before meals and after toilet use. In
nursing homes, the residents are responsible for their
own hand hygiene, but at the geriatric ward the health-
carers had to ensure proper hand hygiene of weak
patients. The healthcarers disinfect their own hands
between each patient visit to avoid the spread of in-
fections, however, it is also important to clean hands
thoroughly with water and soap. We observed that
the healthcarers tend to disinfect their hands instead
of washing, as this is faster.
Potential Use Case: Mobile Hand Disinfection
A mobile robot drives into the patients’ rooms and
offers disinfection of hands. The patients place their
hands in robot and disinfection is sprayed directly on
patients’ hands. An important feature of the robot is
that it motivates/nudge the patients to disinfect hands.
These 5 early use cases were introduced to a fo-
cus group in a Danish hospital and a German nursing
home. The group of Healthcare professionals quali-
fied and ranked the use cases with regard to impor-
tance. Based on the inputs from the focus group, two
use cases were chosen. Use case 1 dispensing of small
equipment and use case 2 tracking of large equipment.
Use case 2 is a non robotic use case consisting of a
Bluetooth tracking system placed on all large equip-
ment in order for healthcarers to track it. In the fol-
lowing only use case 1 will be focused on.
Use Case 1 Flow: Mobile Robot Dispensing Small
Equipment
The goal of the use case is to support the care staff
by giving them a storage room on wheels, that is al-
ways where it’s needed with needed equipment. All
the necessary equipment are sterile and/or clean, until
they are pulled from the dispenser. The flow of the
use case is outlined below:
1. The robot is filled with the required items in the
central storage.
2. The robot drives to its designated department and
positions itself centrally in the corridor.
3. The robot can be called to the entrance of a patient
room using call buttons installed in each room.
4. When the robot arrives the nurse is informed and
the necessary items from the robot can be taken.
In the following section, a description of the tests
process of the Health-CAT robot is given.
4.3 The Test Process
Three rounds of tests in the geriatric ward at SHS
Aabenraa have been conducted. The testing consisted
of two, one-day long mock-up tests and final test with
the developed prototype that spanned a full week.
The goal is to verify in the clinical setting that the
robot complies with the use case and to document
the effects of its use. With each test a new iteration
of the robot has been developed, incorporating find-
ings of the earlier tests and progressing from a simple
mock-up to an actuated robot. We started with some-
thing very simple and then in each test iteration, we
added more technical details. Thereby We avoided the
Health-CAT: Development of a Mobile Robot for Assisting Caregivers
175

Figure 3: Timeline of the development and test cycles in Health-CAT with three different prototypes: a passiv mockup (left),
a mockup with relevant sensor capabilities and user interfaces (center), and the final, actuated prototype.
robot getting a negative reputation early and the work-
flow being altered drastically before we knew that we
could technically solve the actual use case. The hos-
pital staff reported, that the existing robot technology
deployed there often also was a nuisance. The way it
behaved was often unclear and we wanted to ensure
the opposite in Health-CAT. Therefore we recorded
data about the environment to be fed into the vision
and navigation system. The hospital employees also
reported fear of losing their jobs to robots. We in-
cluded them after each test iteration. This made the
users feel ownership of the robot since they were part
of the development process and we could continu-
ously explain and show them that this robot was a tool
for them and not a replacement. On figure 3 a time-
line of the overall test process in Health-CAT can be
seen. In the following, a general description of the
test process is listed.
4.3.1 Mock-up 1 and 2
The first two mock-up tests were designed as non
robotic and was situated at the geriatric ward at SHS
Aabenraa. A nurse was pushing a drawer on wheels
and together they functioned as the robot, see fig-
ure 3. In mock-up test 1 we did some very basic
and early testing, we installed Bluetooth buttons in
half of the patient rooms at the ward. These buttons
was connected to a similar Bluetooth button outside
the room that was visually on the hallway, when the
button inside the patient room was pushed, the but-
ton outside lighted up with green light, and the nurse
acting as the robots actuators pushed the mock-up to
the specific room. The testing was done during the
morning round, afternoon round and during the night
shift. The flow of the mock-up test basically follow
the earlier described use case; when a nurse enters
a patient room, the installed button was clicked and
the button outside the patient room lighted green, re-
sembling that the robot was notified that this specific
room needed equipment. The nurse controlling the
”robot” would then drag the drawer to the specific
room that lighted green. This early mock-up test was
primarily conducted to get a general understanding of
how this robot solution could be build and how it po-
tentially would affect the workflow. Interviews with
the staff involved in the mock-test was conducted and
data from this was feed into the following testing.
Mock-up test 2 is an extension of the first test, see
figure 3. We performed the test on the full ward in-
cluding every patient room. We automated more fea-
tures in the process such as the calling system. We
added a feedback mechanism on the button so the
nurses could see that the robot is on its way and that
the robot has arrived outside the patient room. We
added visual feedback (LED strip around the robot)
that indicates the internal state of the robot, blue when
it drives and green when it can be accessed by a nurse.
We added later a laser scanner and a camera hub on
top of the robot so we could gain data about the real
environment to use for improving and developing our
navigation system. Again, interviews with the staff
involved in the mock-test was conducted and data
from this was feed into development of the prototype.
4.3.2 Prototype Test
The final test was also performed at the geriatric ward
at SHS Aabenraa. The Robot prototype shown on fig-
ure 4 was tested for 1 week during every shift of the
day. In this test we focused on measuring and ob-
serving the general work processes and compare it to
data collected during our field work. Some of the core
findings are listed below:
• Change in Nurse Walking Distance: One of the
core findings was that the nurses took way less
HUCAPP 2022 - 6th International Conference on Human Computer Interaction Theory and Applications
176

steps during a work day working with the robot
vs not having the robot.
• Change in Used Time Picking up Equipment:
There was a large time save in picking up equip-
ment and they spend less time locating equipment.
• The General Flow of Their Work with a Robot:
Several nurses reported an increase of empower-
ment and that the environment was less hectic in
general since the robot was always at the right
place at the right time. The risk of spreading in-
fections was considered reduced using the robot.
• Change in Disturbances from Other Employ-
ees: The nurses were disturbed less by each other
and therefore more time was spend with the pa-
tients.
• Use of Freed up Time: We measured that the
nurses spend more time in the patient rooms.
5 ROBOT PROTOTYPE
The robotic system consists of two major parts – a
robot prototype and a call system – which both con-
sists of various subcomponents. The prototype con-
sists of a mobile base, a cabinet, a GUI head, and a
handle for manual movement of the robot in emer-
gency situations (see fig. 4). The base has two ac-
tuated differential drive wheels in the middle of the
base, and two safety lasers in opposite corners. The
cabinet is made by Standard Systemer
2
and is ap-
proved for clinical use. The two narrow sides of the
cabinet (front and back of the robot) each has a Re-
alSense D415
3
RGB-D sensor, which are used for de-
tecting people in the hospital hallways. The GUI head
has a screen which is used to show the control inter-
face for the robot. It also contains processing units
for sensor processing and robot control. The handle
is attached to the brake system and disengages the
brakes when pulled, which allows for manual move-
ment of the robot. The robotic prototype is based on
ROS (Quigley et al., 2009) and uses the ROS naviga-
tion stack (Marder-Eppstein et al., 2010) for navigat-
ing the hallways of the hospital.
The call system consists of WiFi enabled buttons
which are placed in each patient room. Once a button
is pressed it transmits a unique ID to the robot through
the MQTT messaging protocol, and the room corre-
sponding to that ID is placed in a queue. An RGB
LED on the button provides feedback to the user: blue
if that room is first in line and yellow otherwise.
When the queue is not empty, a navigation goal
in front of the door to the patient room at the top of
2
https://standardsystem.dk/
3
https://www.intelrealsense.com/depth-camera-d415/
Figure 4: Final prototype that has been evaluated.
the queue is sent to the navigation stack. While nav-
igating to the room the robot detects and tracks peo-
ple in the hallway (Juel et al., 2020), and the tracked
people are used as input to a social navigation behav-
ior (Haarslev et al., 2021). The tracker is based on
the CenterNet (Zhou et al., 2019) human pose estima-
tion network and the Deep SORT (Wojke et al., 2017)
object tracker. The system works by feeding images
from the two cameras to the human pose estimator,
which estimates bounding boxes and joint locations
for each person in the view. The joints are projected to
3D, and the torso center and facing direction of each
person is estimated using the 3D shoulder joints. The
pose is transformed to the map frame using localiza-
tion data from the navigation stack. The transforma-
tion to the map frame serves two purposes: it uni-
fies the detection frames from the two cameras, and it
eliminates the problem of egomotion when tracking.
The transformed detections are used as input to a
modified Deep SORT algorithm. Deep SORT tracks
objects based on deep appearance features found by
inputting images of each detected person to a Siamese
CNN trained with triplet loss (Schroff et al., 2015). It
incorporates a Kalman filter , which predicts the mo-
tion of the tracked people. A cost matrix is created
using the distance between the deep appearance fea-
tures of the tracks and the new detections. The cost
matrix is gated by setting costs to infinity for detec-
tion/track pairs where the detection is too far away
from the predicted position of the track. Association
is done by solving the cost matrix using the Hungar-
ian algorithm. The Deep SORT algorithm is modified
by changing the state space of the Kalman filter from
image coordinates to 3D map frame coordinates.
The tracked people are input to a social navigation
method, which is integrated with the ROS navigation
stack. The method works by creating costs represent-
ing social spaces (Lindner and Eschenbach, 2011) at
estimated collision points between the robot and the
Health-CAT: Development of a Mobile Robot for Assisting Caregivers
177

tracked people. The collision points are estimated us-
ing the tracked motion of the people, and the motion
of the robot. By projecting costs to future positions of
the people the robot preemptively avoids entering the
personal space of the people, resulting in a socially
acceptable navigation behavior.
6 CONCLUSIONS
We have described the process of developing a robot
to solve a use case within healthcare. The goal of
the Health-CAT project is to ensure that the quality of
care does not decrease despite the healthcare system
being challenged due to the expected issues arising
from the societal challenges. This process is based
on a needs analysis using literature search and ethno-
graphic studies to identify relevant focus areas. From
these needs, seven use cases were formulated with
ethical and technical challenges, concerning the im-
plementation and introduction of robot technology, as
a focus point. We ended up choosing one use case, the
transportation of small equipment, where the robotic
system consists of two major parts - a mobile robot
prototype and a call system enabled staff to call the
robot to any patient room.
This robot concept was tested in three iterations.
The first two iterations were highly focused on iden-
tifying the requirements, issues, and benefits of the
robot. The last test involved the actual robot proto-
type in a one-week-long integration of it at the hos-
pital ward. The Health-CAT robot showed that the
daily work life for nurses improved. They walked
less, which decreased the physical stress, and experi-
enced an increase of the time spent with the patients.
Furthermore, nurses reported an increase in perceived
empowerment and that their work environment was
less hectic in general.
ACKNOWLEDGEMENTS
This research was supported by the project Health-
CAT, funded by the European Fund for regional de-
velopment.
Furthermore we would like to thank the involved
staff at the Hospital Sønderjylland, UKSH L
¨
ubeck
and AWO Haus am M
¨
uhlenteich Lensahn for their
valuable input and support.
REFERENCES
Bodenhagen, L., Suvei, S.-D., Juel, W. K., Brander, E.,
and Kr
¨
uger, N. (2019). Robot technology for future
welfare: Meeting upcoming societal challenges – an
outlook with offset in the development in scandinavia.
Health and Technology.
Cresswell, K., Cunningham-Burley, S., Sheikh, A., et al.
(2018). Health care robotics: qualitative exploration
of key challenges and future directions. Journal of
medical Internet research, 20(7).
Drennan, V. M. and Ross, F. (2019). Global nurse shortages:
The facts, the impact and action for change. British
medical bulletin, 130(1):25–37.
Falatah, R. (2021). The impact of the coronavirus disease
(covid-19) pandemic on nurses’ turnover intention:
An integrative review. Nursing Reports, 11(4):787–
810.
Haarslev, F., Juel, W. K., Kollakidou, A., Kr
¨
uger, N., and
Bodenhagen, L. (2021). Context-aware social robot
navigation. In ICINCO.
Holland, J., Kingston, L., McCarthy, C., Armstrong, E.,
O’Dwyer, P., Merz, F., and McConnell, M. (2021).
Service robots in the healthcare sector. Robotics,
10(1).
International Federation of Robotics (2020). World
Robotics (Summary). VDMA, Frankfurt am Main,
Germany.
Juel, W. K., Haarslev, F., Kr
¨
uger, N., and Bodenhagen, L.
(2020). An integrated object detection and tracking
framework for mobile robots. In ICINCO.
Lindner, F. and Eschenbach, C. (2011). Towards a formal-
ization of social spaces for socially aware robots. In
Spatial Information Theory, pages 283–303.
Marder-Eppstein, E., Berger, E., Foote, T., Gerkey, B. P.,
and Konolige, K. (2010). The office marathon: Ro-
bust navigation in an indoor office environment. 2010
IEEE Int. Conf. on Robotics and Automation.
OECD (2014). Health expenditure indicators.
Quigley, M., Gerkey, B., Conley, K., Faust, J., Foote, T.,
Leibs, J., Berger, E., Wheeler, R., and Ng, A. (2009).
Ros: an open-source robot operating system. In Proc.
of the IEEE Intl. Conf. on Robotics and Automation;
Workshop on Open Source Robotics.
Radic, M., Vosen, A., and Graf, B. (2019). Use of robotics
in the german healthcare sector. In Social Robotics,
Cham. Springer International Publishing.
Schroff, F., Kalenichenko, D., and Philbin, J. (2015).
Facenet: A unified embedding for face recognition
and clustering. 2015 IEEE Conference on Computer
Vision and Pattern Recognition.
Stahl, B. C. and Coeckelbergh, M. (2016). Ethics of health-
care robotics: Towards responsible research and inno-
vation. Robotics and Autonomous Systems, 86.
Wojke, N., Bewley, A., and Paulus, D. (2017). Simple on-
line and realtime tracking with a deep association met-
ric. In 2017 IEEE Int. Conf. on Image Processing.
Zhou, X., Wang, D., and Kr
¨
ahenb
¨
uhl, P. (2019). Objects as
points. ArXiv, abs/1904.07850.
HUCAPP 2022 - 6th International Conference on Human Computer Interaction Theory and Applications
178
