
An Assistive Technology for Cognition to Support Meal Preparation:
The Concept Map of a User-centred Design Process and Procedure
Sareh Zarshenas
1,2 a
, Nathalie Bier
1,3 b
, Helene Pigot
4
, Sylvain Giroux
4
c
,
Patricia Briskie Semeniuk
2
, Melanie Couture
4
and Carolina Bottari
1,2
d
1
Occupational Therapy Program, School of Rehabilitation, Universite de Montreal, Montreal, Canada
2
Centre for Interdisciplinary Research in Rehabilitation of Greater Montreal, Canada
3
Centre de Recherche de’Institut Universitaire de Geriatric de Montreal, Montreal, Canada
4
Universite de Sherbrooke, Sherbrooke, Canada
{helene.pigot, sylvain.giroux, melanie.couture}@usherbrooke.ca
Keywords: User-centred Design, Assistive Technology, Cognition, Activity of Daily Living, Meal Preparation, Acquired
Brain Injury, Concept Map.
Abstract: In response to the long-lasting effects of cognitive impairments following acquired brain injury (ABI) on
performing meal preparation safely and independently, our team has been working on developing a Cognitive
Orthosis for coOKing (COOK) to meet these needs. In this paper, the concept mapping method was used to
describe the processes and procedures of employing a user-centred design approach to develop this novel
technology. For this purpose, a mixed methodology including qualitative and quantitative studies was
conducted for needs analysis, prototype design, prototype evaluation, and technology validation via the
examination of the usability and feasibility of COOK within real-life contexts. Our comprehensive studies
have shown that COOK is a promising technology for meal preparation by individuals with severe ABI.
Further study is warranted/in progress to develop a therapist’s interface to tailor the required type and level
of assistance to a broader population with cognitive deficits of varying severity.
1 INTRODUCTION
Cognitive impairments following acquired brain
injury (ABI), may significantly affect cognitive
domains such as executive functions (Funahashi S &
Andreau JM, 2013). Executive functions are higher-
level cognitive functions necessary for directing
actions to perform instrumental activities of daily
living (IADL) (Blomgren C, & et al., 2019; Crichton
SL, & et al., 2016; Diamond A, 2013; Zinn D, & et
al., 2004). Meal preparation is a complex IADL that
heavily draws on executive functions and is essential
for living independently (Doherty TA, & et al., 2015;
Godbout L, & et al., 2004; Tanguay AN & et al.,
2014). Long-lasting effects of executive function
deficits in individuals with ABI may contribute to
difficulties in the meal preparation process, including
a
https://orcid.org/0000-0002-2872-3257
b
https://orcid.org/0000-0002-2440-694X
c
https://orcid.org/0000-0003-0602-5957
d
https://orcid.org/0000-0003-2242-8369
setting goals, planning steps, initiating meal
preparation, monitoring actions, and inhibiting
inappropriate behaviors (Bottari C, & et al., 2009;
Doherty TA et al., 2015; Tanguay AN et al., 2014).
With the evolution of smart technologies,
assistive technologies for cognition (ATC) are
strategically positioned to enhance healthcare
services and enable people with cognitive
impairments to be more independent in their daily
living activities such as meal preparation (Jamieson
M & et al., 2020; WHO, 2015). ATCs refer to
“technologies that enable, enhance, or extend
cognitive function in which the human user is an
autonomous agent using tools to facilitate their
cognition” (O'Neill B & Gillespie A, 2014). Over the
last decade, there has been a growing body of
evidence about the potential of ATCs in enabling
Zarshenas, S., Bier, N., Pigot, H., Giroux, S., Semeniuk, P., Couture, M. and Bottari, C.
An Assistive Technology for Cognition to Support Meal Preparation: The Concept Map of a User-centred Design Process and Procedure.
DOI: 10.5220/0010933900003123
In Proceedings of the 15th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2022) - Volume 5: HEALTHINF, pages 921-928
ISBN: 978-989-758-552-4; ISSN: 2184-4305
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
921

individuals with ABI to actively engage in daily
activities while supporting formal and informal
caregivers (Jamieson M, et al., 2020; Kettlewell J, &
et al., 2019; Leopold A, & et al., 2015; Nam J, & Kim
H, 2018; Vaezipour A, & et al., 2019; Wang J, & et
al., 2016; Widehammar C, & et al., 2019). Among
different categories of ATCs that focused on
executive functions, most are designed to help with
time management (i.e., reminding, and scheduling
technologies) or developed to assist with guiding
people through tasks (i.e., micro-prompting systems
that support multi-step task performance) (Mihailidis
A, & et al, 2008; O'Neill B & Gillespie A, 2014;
Rudzicz F, & et al., 2015). However, very few of
these technologies include a consideration of
assisting with the multiple aspects of executive
functions in complex tasks (e.g., setting a goal,
organization and problem-solving, preventing
hazardous behaviors, completing the task, and
evaluation of the outcome), which are inherent to
meal preparation (Wang J, & et al., 2019).
To propose a technological solution to target
various aspects of executive dysfunctions while
simultaneously improving independence and safety
in meal preparation, our interdisciplinary team has
been working on developing an ATC called
“Cognitive Orthosis for coOKing” (COOK) (Giroux
S, & et al., 2015; Olivares M, & et al., 2019;). COOK
is a web-based and context-aware system that was
developed based on the user-centred design (UCD)
approach in the context of a living lab (Pinard S, & et
al., 2019). COOK has three main components: 1) a
sensor-based security system to monitor safety
incidents via different types of sensors such as motion
detectors, pressure and infrared sensors, developed
based on a preventive assistance model (Olivares M,
& et al., 2016); 2) a cognitive assistance application
to increase independence providing step by step
instruction in the process of meal preparation via a
touch screen tablet and supporting executive function
sub-skills of setting a goal, planning steps, choosing
a recipe, following instructions, adjusting a reminder,
completing a task, and goal attainment evaluation;
and 3) a configuration system that makes it possible
to tailor COOK’s features to the individuals’ needs
while also providing accessibility to COOK’s activity
log (e.g., type of errors that occurred in conforming
safety rules) by expert clinicians, ideally occupational
therapists (OTs) (figure 1). Also, an extra screen can
be installed in the caregivers/ therapists’ room to
inform them of the stove’s/oven’s status (on/off) and
possible safety issues occurring while in use
(dashboard). In this manuscript we aimed to provide
a comprehensive overview of our projects to develop
and validate COOK.
2 METHODS
To meet the objective of this study, we used concept
mapping as a structured methodology for illustrating
steps and employed procedures within the UCD
process to explain the whole procedure of designing,
examining COOK’s usability, and implementing of
COOK within real life contexts (figure 2) (Kane,
2007). This method includes an integrated mixed
method of qualitative and quantitative data collection
that enabled us to access in-depth knowledge from
various stakeholders. Comprehensive information on
the methodologies used for conducting studies at the
different steps of the USD process are provided in the
following sections.
Figure 1: COOK Hardware Components.
Smart CommuniCare 2022 - Special Session on Smart Living Environments to Support Aging-in-Place in Vulnerable Older Adults
922
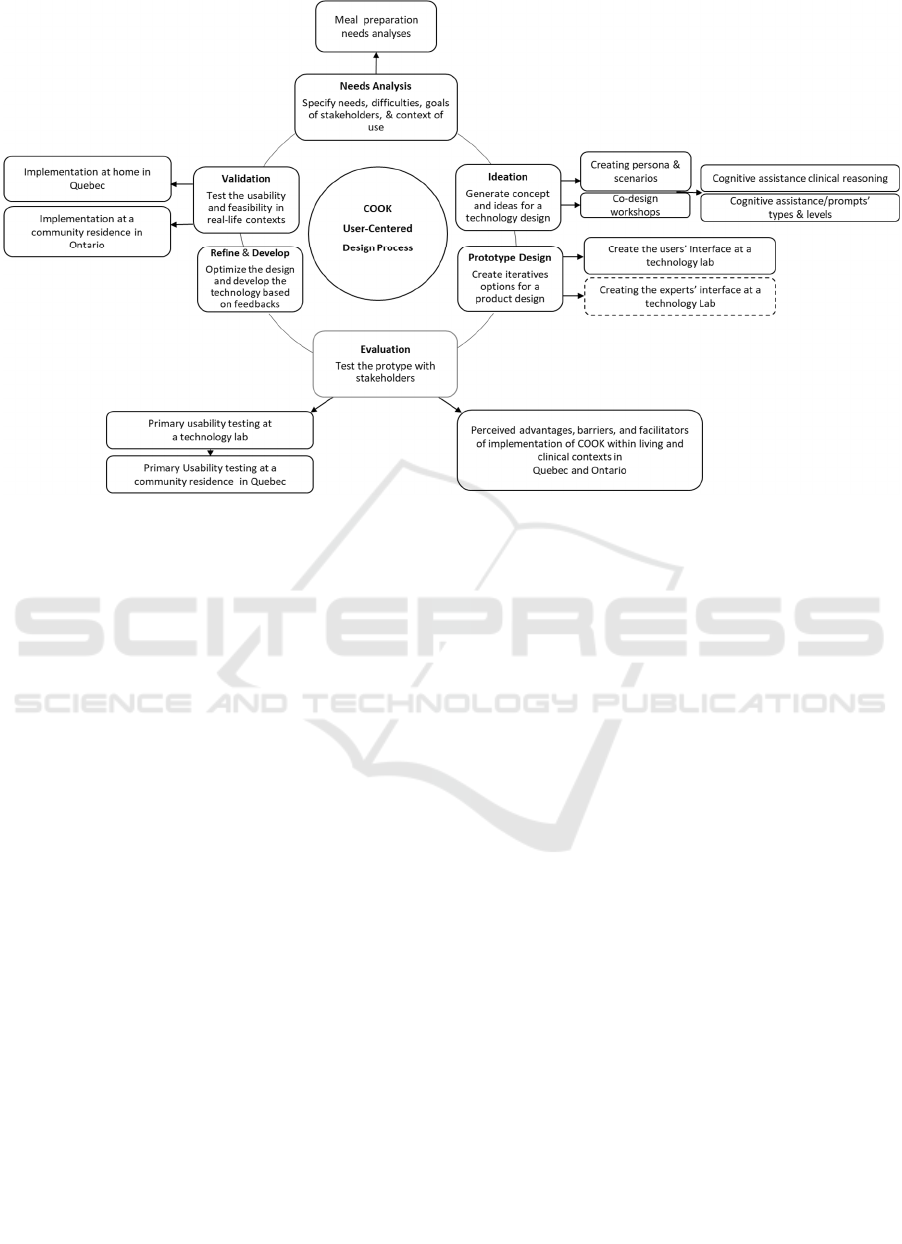
Figure 2: User-Centred Design Concept Map.
3 USER-CENTRED DESIGN
PROCESS, PROCEDURES, AND
RESULTS
UCD is an evidence-based and iterative approach that
incorporates the needs and context of a specific end-
user group and helps ensure that an invented and
novel technology is acceptable and effective (User-
Centered Design Basics, accessed October 2021).
3.1 Needs Analysis
To design an ATC that facilitates meal preparation for
individuals with ABI, one of the imperative steps is
to explore the main requirements and difficulties of
these individuals and other stakeholders in various
processes of meal preparation considering the
interaction of personal, environmental, and task
related factors (Dubuc E, & et al., 2019; Gagnon-Roy
M, & et al., 2020; Pinard S & et al., 2019; Zarshenas
S, & et al., 2020, 2021). For this purpose, descriptive
qualitative studies were conducted by carrying out
interviews and focus groups with individuals with
ABI (n=20) particularly traumatic brain injury
(n=14), their caregivers (n=13), and health care
providers (n=30) and assessing individuals’ level of
independence in meal preparation using the IADL
Profile (n=3) (Dubuc E & et al, 2019; Gagnon-Roy M
et al., 2020; Pinard S & et al., 2019; Zarshenas S et
al., 2020, 2021). Also, as another component of need
analysis, clinical reasonings to provide various levels
of verbal assistance by OTs (n=3) were investigated
via performing IADL Profile to inform the computer
scientists regarding the process of integrating the
verbal assistance within the design of COOK’s
cognitive assistance (Gagnon-Roy M, & et al., 2021).
Findings of these studies revealed various needs and
difficulties in four main areas regarding meal
preparation including psychosocial, cognitive, and
physical abilities, and environment characteristics.
With respect to the psychosocial aspect,
motivation to initiate the task, ability to maintain the
energy level required to engage in the task following
the onset of fatigue, need to change old habits in meal
preparation that may no longer be adapted to the
person’s abilities, managing impulsive behaviors, and
availability of caregiver’s support were all considered
necessary to engage in the meal preparation task
(Dubuc E, & et al, 2019; Zarshenas S, & et al., 2020,
2021).
Regarding cognitive and executive function,
difficulties in formulating a goal, planning, and
carrying out the task, problem solving, tailoring the
meal preparation process to the person’s cognitive
abilities were mentioned as important factors that
may limit the ability to complete the task safely and
independently (Dubuc E, & et al, 2019; Gagnon-Roy
An Assistive Technology for Cognition to Support Meal Preparation: The Concept Map of a User-centred Design Process and Procedure
923

M, et al., 2020; Pinard S, & et al., 2019; Zarshenas S,
et al., 2020, 2021).
Further, adaptation of the meal preparation task to
individuals’ fine and gross motor abilities were
mentioned as another necessary element to carrying
out the meal preparation task in a safe manner (Dubuc
E, & et al, 2019; Gagnon-Roy M, et al., 2020; Pinard
S, & et al., 2019; Zarshenas S, et al., 2020, 2021).
Finally, the level of support that could be provided
within a living environment (home vs. supported
residence) was considered as a determining factor to
perform the meal preparation task successfully
(Dubuc E, & et al, 2019; Gagnon-Roy M, et al., 2020;
Pinard S, & et al., 2019; Zarshenas S, et al., 2020,
2021). Stakeholdrs also expressed that available
commercial products have not been designed
specifically to meet the needs of individulas with
ABI which imposes a significant burden on
caregivers who have to provide personalized
cognitive assistance (e.g., verbal and visulal) to
compensate the cognitive and excecutive
impairments for their loved ones (Zarshenas S, et al.,
2020, 2021). Also, our findings showed that four
factors may affect providing verbal assistance
including presence of safety and emotional issues,
lack of progress in the task, requests for support, and
off-task discussions (Gagnon-Roy M, & et al., 2021).
3.2 Ideation
After obtaining in depth knowledge regarding the
needs and preferences of stakeholders, an
interdisciplinary team including rehabilitation (n=4)
and computer scientists (n=2), clinicians (n=3, OTs),
and potential end-users (n=3) collaborated to
brainstorm ideas to design different components of
COOK (Pinard S & et al., 2019;). Various strategies
were used to facilitate this step comprising persona
and scenario creation, ideation workshops, and co-
designing workshops (Olivares M, & et al., 2020;
Pinard S & et al., 2019).
As part of the UCD process, persona and scenarios
were used to characterize archetypes of various end
users to facilitate the interdisciplinary collaboration
between clinicians, computer scientists, and other
stakeholders. Personas and scenarios were created
through interdisciplinary workshops and video
analysis of individuals with traumatic brain injury
(n=4) being tested with the IADL Profile evaluation
by an OT.
As a result of this study, personas and scenarios
were created including individuals’ demographic and
clinical profiles and the types and levels of cognitive
assistance provided by OTS to facilitate the meal
preparation task for these personas. In total, three
personas were developed for mild, moderate, and
severe traumatic brain injury (TBI).
These personas were used in co-designing
workshops with various stakeholders to inform how
certain features should be designed or integrated to
meet end-user’s needs particularly in the client’s
interface of COOK. As part of the ideation and co-
designing workshops, several multidisciplinary team
meetings were held regarding strategies to maximize
safety and facilitate cognitive difficulties during meal
preparation that helped with the COOK mock-up
ideas (Pinard S, & et al., 2019).
3.3 COOK Iterative Prototype Design
The design process of COOK was iterative and
incremental with new features added gradually over
the course of several different studies. The design
team that remained stable throughout all stages of the
design process included computer scientists, OTs, a
psychologist, an implementation science expert, and
potential end-users including individuals with a
moderate to severe TBI (Pinard S, et al., 2019).
The interactive prototype was designed
progressively through simulating features and
functions via an interdisciplinary collaboration and
applying qualitative feedback from end-users
regarding their interaction with features and functions
to improve simulated features. During these sessions,
various strategies such as interviews, storyboarding,
scenario testing, and Wizard of Oz were used for the
iterative and incremental development process to
design the COOK interface for individuals with ABI
(Pinard S, & et al., 2019).
3.4 Evaluation of the COOK Prototype
To evaluate the prototype, different techniques were
used including cognitive walk-through, lab testing of
usability, and field testing of usability.
3.4.1 The Cognitive Walk-through
The cognitive walk-through method is “a usability
evaluation method in which one or more evaluators
work through a series of tasks and ask a set of
questions from the perspective of the user” (Usability
Body of Knowledge, accessed December 2021). For
this purpose, we carried out interviews and focus
groups with various stakeholders including
individuals with moderate to severe ABI (n=20),
caregivers (n=13), and health care providers (n=30).
They were provided a short demo of COOK’s
Smart CommuniCare 2022 - Special Session on Smart Living Environments to Support Aging-in-Place in Vulnerable Older Adults
924

features and functions to enable them to provide
feedback on the perceived advantages, barriers, and
facilitators to implementing COOK within living and
clinical contexts (Gagnon-Roy M, & et al., 2020;
Zarshenas S, & et al., 2020, 2021).
Findings showed that participants perceived
COOK as a promising technology to improve
independence and safety in meal preparation in the
ABI population while addressing caregivers’ burden
of care. For instance, availability of various types of
recipes with different levels of complexity, lists of
ingredients for each recipe, weekly meal, and grocery
planner, step by step instructions, portability, and
possibility of installing COOK on various electronic
stoves were all reflecting the positive potential of this
technology. However, limited access to financial
resources or funding to cover the cost of purchasing
technology, being trained on, and using COOK,
severity of injury, cognitive impairments and
psychosocial deficits, absence of supportive
caregivers, and some gaps in COOK’s software (e.g.,
not designed for multiple users, not accessible in all
languages) and hardware (e.g., not designed for a gas
stove) of the technology were described as the main
barriers that needed to be addressed to scale the
implementation of COOK. Further, raising awareness
about COOK, providing training to end-users and
their caregivers/providers, and availability of
technical support were considered as facilitators to
the eventual widespread implementation of COOK
and address some of the perceived barriers.
3.4.2 The Lab Testing of Usability
The primary version of technology was evaluated by
conducting two rounds of usability and user
experience (UX) evaluations which were completed
in a laboratory context including 3 sessions with 5
experts and 2 sessions with 10 TBI participants. Lab
usability tests measure a user's ability to complete
tasks (Usability Body of Knowledge, accessed
December 2021). Examination of the usability in the
lab, provided us with an opportunity to involve more
participants to ensure the reliability of the results
(Gagnon-Roy M, & et al, 2021, submitted).
Each session included the use of scenarios and
questionnaires regarding the users’ experience and
the technology’s usability. The UX and usability
evaluations of the user interface components of
COOK were completed via three steps: 1) a general
presentation of COOK, 2) simulating the use of the
technology via scenarios, and 3) administration of
two questionnaires; the System Usability Scale and
the Attrak-Diff Scale (Brooke J, 1996; Lallemand C,
& et al., 2015). During each simulation, participants
were asked to describe their thoughts using a think
aloud process, explaining their understanding of the
task and the technology, and comment on the
technology’s ease of use and potential. Both rounds
demonstrated good usability outcomes and good
hedonic qualities. Various usability issues were
identified by participants, such as navigation
inconsistencies and technical bugs. Factors to
consider in the future implementation of COOK were
also mentioned by TBI participants, including
environmental and personal factors (e.g., level of
comfort using the technology, and possible impact of
visual deficits on use of the technology).
3.4.3 The Field Testing of Usability
To test a product in the actual context, we used field
usability testing (Usability Body of Knowledge,
accessed December 2021). Considering the lessons
learned from the lab testing of COOK, we continued
to evaluate the usability of a modified version of
COOK over a 6-month period for 3 individuals with
severe TBI, with an average of 22 years post-injury,
through evaluating effectiveness, efficiency, and
satisfaction. This study took place at a community
residence in Sherbrooke where we made a partnership
to run the COOK project and expand our study scope.
Results of effectiveness and efficiency evaluation
revealed that the number of meals prepared with
COOK’s support increased significantly over time
while safety warnings and automatic stove shot
downs by the autonomous safety system decreased
over time. As part of the design process, technology
bugs and malfunctions (e.g., false alarms, sensitivity
of sensors) were precisely documented and prototype
modifications and refinements were made (Pinard S,
& et al., 2019). Further, findings highlighted the
importance of considering training as an imperative
complementary component to use COOK over
extended period by individuals with TBI.
3.5 Refinement and Development of the
Prototypes
While refinement and modification of the technology
was considered as an ongoing process during the
course of developing COOK, and after lab and field
testing of its usability, the interdisciplinary team
continued working on COOK to advance both French
and English versions of it, removing bugs, setting a
technical support team, and creating a light and
portable version to make it prepare for usability and
An Assistive Technology for Cognition to Support Meal Preparation: The Concept Map of a User-centred Design Process and Procedure
925

feasibility testing within real-life contexts in Quebec
and Ontario.
3.6 Validation
To validate the usability and feasibility of COOK
within real-life contexts, COOK was implemented at
a shared community residence for a 47-year-old
woman with chronic severe stroke (C1) in Ontario
and within the home of a 35-year-old man with
chronic severe TBI in Quebec, Canada (C2) (Gagnon-
Roy M, & et al., 2021, submitted; Zarshenas S, & et
al., 2021).
For both studies we used a mixed-methods single
case design, including a multiple baseline single-case
experimental study and a descriptive qualitative study
(Onghena P, & et al., 2018). C1 received
comprehensive training on using COOK within a
shared kitchen space at the residence. During meal
preparation, independence and safety were evaluated
using three target behaviors: required assistance, task
performance errors, and appropriate responses to
safety issues, which were compared with an untrained
control task, making a budget. Benefits, barriers, and
facilitators were assessed via three individual
interviews with the client and three focus groups with
the care team before, during and after the COOK
implementation. For C2, target behaviors included
the number of meals prepared each week using
COOK, and indicators of performance during both a
meal preparation task and a control task, obtaining
information. Both quantitative and qualitative
analyses of C1 data showed that COOK significantly
increased independence and safety during meal
preparation. No changes were observed in the control
task. Stakeholders suggested that the availability of a
training toolkit would facilitate the involvement of a
greater number of therapists at the residence and the
installation of COOK within the client’s own
apartment would help with the successful adoption of
this technology (Zarshenas S, & et al., 2021). Also,
C2 showed an improved ability to prepare meals
overtime with less assistance being required and a
more efficient preparation of meals using COOK
(Gagnon-Roy M, et al., 2021, submitted). Comparing
the results of these two studies showed that a client
who was surrounded by a team of care at the residence
could receive more support than a client who lived at
home. However, both clients and care
providers/givers comprehended COOK as an
effective technology to increase independence of
clients with ABI (Gagnon-Roy M, & et al., 2021,
submitted; Zarshenas S, & et al., 2021).
4 CONCLUSION AND FUTURE
DIRECTIONS
To our knowledge, COOK is the first assistive
technology for cognition, designed for performing
meal preparation task by individuals with a severe
ABI. Our current studies showed the successful
usability and feasibility examination of this
technology particularly for individuals with severe
ABI. However, considering the variation of ABI
individuals’ needs based on their severity of injury
and cognitive impairments, our team is presently
working on developing the expert interface as part of
the configuration system where therapists will have
the possibility of adjusting the types and levels of
cognitive assistance provided by the technology’s
prompts to expand the usefulness of this technology
for a broader population with ABI with various level
of cognitive functions. In line with this goal, our
interdisciplinary team is also collaborating with OTs
to translate their clinical reasonings regarding types
and levels of cognitive assistance to appropriate
visual and verbal prompts within the configuration
system in COOK to meet the individuals’ needs
during meal preparation (Tekemetieu A, & et al, in
preparation). Finally, to explore application of COOK
to a broader population, we are exploring the
implementation of COOK for older adults with mild
cognitive impairments. Preliminary findings
indicated the potential of COOK for this population
(Yaddaden A, & et al., 2020). Further studies are
warranted regarding the usability and feasibility of
this technology for the aging population.
ACKNOWLEDGEMENTS
We would like to gratefully acknowledge all
participants who assisted in making this work a
reality. This project was funded by Canadian
agencies: Canadian Institute of Health Research,
National Sciences and Engineering Research Council
of Canada, ONF-REPAR, OPHQ-REPAR, AGE-
WELL, and the CRIUGM. N.B. is supported by a
salary award from the Fonds de la recherche du
Quénec – Santé.
REFERENCES
Blomgren C., Samuelsson H., Blomstrand C., & et al.
(2019). Long-term performance of instrumental
activities of daily living in young and middleaged
Smart CommuniCare 2022 - Special Session on Smart Living Environments to Support Aging-in-Place in Vulnerable Older Adults
926

stroke survivors-Impact of cognitive dysfunction,
emotional problems and fatigue. PLOS ONE, 14(5), 1-
14.
Bottari C., Dassa C., Rainville C., & et al. (2009). The
factorial validity and internal consistency of the
Instrumental Activities of Daily Living Profile in
individuals with a traumatic brain injury.
Neuropsychological Rehabilitation, 19(2), 177-207.
Brooke J. (1996). SUS: A quick and dirty usability scale.
London:: Taylor & Francis.
Crichton SL, Bray BD, McKevitt C, & et al. (2016). Patient
outcomes up to 15 years after stroke: survival,
disability, quality of life, cognition and mental health. J
Neurol Neurosurg Psychiatry(87), 1091-1098.
Diamond A. (2013). Executive Functions. Annu Rev
Psychol, 64:, 135–168.
Doherty TA, Barker LA, Denniss R, & et al. (2015). The
cooking task: making a meal of executive functions
Frontiers in Behavioral Neuroscience, 9, 1-10.
Dubuc E, & et al. ( 2019). Perceived needs and difficulties
in meal preparation of people living with traumatic
brain injury in a chronic phase: Supporting long-term
services and interventions. Australian Occupational
Therapy Journal, 66, 720-730.
Funahashi S, & Andreau JM. (2013). Prefrontal cortex and
neural mechanisms of executive function. . J Physiol
Paris, 107(6), 471-482.
Gagnon-Roy, Bier N, Boulé-Riley S, & et al. (2021).
Providing Verbal Assistance When Assessing
Individuals Living with a Traumatic Brain Injury.
Canadian Journal of Occupational Therapy, 1-13.
Gagnon-Roy M, Bier N, Couture M, et al, & ., J.
(2021(submitted)). Usability of an assistive technology
forcognition to support meal prepartion following a
severe traumatic brain injury: A signle-case
exprimental study in a real world environment.
Neuropsychological Rehabilitation.
Gagnon-Roy M, Bier N, C. & et al. (2020, published
online). Facilitators and obstacles to the use of a
cognitive orthosis for meal preparation within the
homes of adults with a moderate to severe traumatic
brain injury: Informal caregivers and healthcare
professionals’ perspectives. Assistive technology: the
official journal of RESNA.
Gagnon-Roy M, Pinard S, Bottari C, & et al. (2021,
submitted). Usability of a smart assistive technology for
cooking (COOK) for people with cognitive
impairments following a traumatic brain injury
Neropsychological Rehabilitation.
Giroux S, Bier N, Pigot H, & et al, C. (2015). Cognitive
assistance to meal preparation: design, implementation
and, assessment in a living lab. AAAI 2015 Spring
Workshop Symposium, Ambient Intelligence for
Health and Cognitive Enhancement,California USA,
pp. 14-16. Technical Report SS-15-01. Published by
The AAAI.
Godbout L, Grenier MC, Braun CMJ, & et al. (2004).
Cognitive structure of executive deficits in patients with
frontal lesions performing activities of daily living.
Brain Injury. ;19(5):, 19(5), 337-348.
Jamieson M, Jack R, O’Neill B, & et al. (2020). Technology
to encourage meaningful activities following brain
injury. Disability and Rehabilitation: Assistiev
Technology, 15(4), 453-466.
Kane M. (2007). Concept Mapping for Planning and
Evaluation, Edited by: Mary Kane & William M.
Trochim Published: 2007.
Kettlewell J, das Nair R, & KA., R. (2019). A systematic
review of personal smart technologies used to improve
outcomes in adults with acquired brain injuries.
Clinical Rehabilitatoin, 33(11), 1705-1712.
Lallemand C, Koenig V, Gronier G, & et al. (2015).
Création et validation d'une version française du
questionnaire AttrakDiff pour l’évaluation de
l’expérience utilisateur des systèmes interactifs.
European Review of Applied Psychology,, 65(5), 239-
252.
Leopold A, Lourie A, Petras H, & et al. (2015). The use of
assistive technology for cognition to support the
performance of daily activities for individuals with
cognitive disabilities due to traumatic brain injury: The
current state of the research. NeuroRehabilitation,
37(3), 359-378.
Mihailidis A, Boger JN, Craig T, & et al. (2008). The
COACH prompting system to assist older adults with
dementia through handwashing: An efficacy study.
BMC Geriatr., 8(28).
Nam J, & Kim H. ( 2018). How assistive devices affect
activities of daily living and cognitive functions of
people with brain injury: a meta-analysis. Disability
and Rehabilitation: Assistiev Technology, 13(3), 305-
311.
O'Neill B, & Gillespie A. (2014). Assistive Technology for
Cognition: A handbook for clinicians and developers:
New York: Psychology Press
Olivares M, Giroux S, De loor P, & et al. (2016). An
ontology model for a context-aware preventive
assistance system: reducing exposition of individuals
with Traumatic Brain Injury to dangerous situations
during meal preparation. 2nd IET International
Conference on Technologies for Active and Assisted
Living.
Olivares M, Pigot H, & Bottari C. (2020). Use of a Persona
to Support the Interdisciplinary Design of an Assistive
Technology for Meal Preparation in Traumatic Brain
Injury. Interacting with Computers, 32(5-6), 435–456.
Onghena P, & et al. (2018). Single Case Research: State of
the Art and Future Directions. Mixed Methods
Research, 13(4), 461-480.
Pinard S, Bottari C, Laliberté C, & et al. (2019;). Design
and usability evaluation of COOK, an assistive
technology for meal preparation for persons with severe
TBI. Disability and Rehabilitation: Assitive technology,
17(1-15).
Rudzicz F, Wang R, Begum M, et al, & ;. (2015). Speech
Interaction with Personal Assistive Robots Supporting
Aging at Home for Individuals with Alzheimer’s
Disease. ACM Transactions on Accessible Computing,
7(2), 1-22.
An Assistive Technology for Cognition to Support Meal Preparation: The Concept Map of a User-centred Design Process and Procedure
927

Tanguay AN, Davidson PSR, Guerrero Nuñez KV, & et al.
(2014). Cooking breakfast after a brain injury.
Frontiers in Behavioral Neuroscience, 8(272), 1-42.
Tekemetieu A, Pigot H, & et al. (in preparation). From
speech acts to assistance acts for cognitive
rehabilitation in ambient assisted living: how to nudge
cognitively impaired people to act independently.
Usability Body of Knowledge. https://www.usability
bok.org/ (accessed December 2021).
User-Centered Design Basics. https://www.usability.gov/
what-and-why/user-centered-design.html (accessed
October 2021).
Vaezipour A, Whelan BM, Wall K, & et al. (2019).
Acceptance of Rehabilitation Technology in Adults
With Moderate to Severe Traumatic Brain Injury, Their
Caregivers, and Healthcare Professionals: A Systematic
Review. J Head Trauma Rehabil, 34(4), E67-E82.
Wang J, Ding D, & Emily E. (2016). Use of Assistive
Technology for Cognition Among People With
Traumatic Brain Injury: A Survey Study. Military
Medicine, 181(6), 560–566.
Wang J, Mahajan HP, & PE., T. (2019). The feasibility of
an automatic prompting system in assisting people with
traumatic brain injury in cooking tasks. Disability and
Rehabilitation: Assistiev Technology, 14(8), 817-825.
WHO global disability action plan 2014-2021: better health
for all people with disability. World Health
Organization. 2015.
Yaddaden A, Couture M, & et al. (2020). Using a cognitive
orthosis to support older adults during meal
preparation: clinicians’ perspective on COOK
technology. Journal of Rehabil Assist Technol Eng. 7,
1-13.
Zarshenas S, Couture M, & et al. (2020). Advantages,
barriers, and facilitators implementing a cognitive
orthosis for cooking for individuals with traumatic
brain injury: the healthcare providers' perspective.
Disability Rehabilitation: Assistive Technology. Nov 5;
1-10.doi: 10.1080/17483107.2020.1833093.
Zarshenas S, Gagnon-Roy M, & et al. (2021). Potential of
using an assistive technology to address meal
preparation difficulties following acquired brain injury:
clients' and caregivers’ perspectives. Disability and
Rehabilitation: Assistive Technology.3(Feb 3),1-9.
Zarshenas S, Couture M, & et al. (2021). Implementation
of an Assistive Technology for Meal Preparation within
a Supported Residence for Adults with Acquired Brain
Injury: A Mixed-Methods Single Case Study. Disability
and Rehabilitation: Assistive Technology. Dec 17:1-17.
doi: 10.1080/17483107.2021.2005163.
Smart CommuniCare 2022 - Special Session on Smart Living Environments to Support Aging-in-Place in Vulnerable Older Adults
928
