
Knowledge Management and Benchmarking for Health Care System
Development Activities
Annamaija Paunu, Hannele Väyrynen and Nina Helander
Information and Knowledge Management, Tampere University, Tampere, Finland
Keywords: Knowledge Management, Benchmarking, Healthcare, Case Study.
Abstract: Knowledge management (KM) has a central role in developing health care services both at the organization
and at the system level. Benchmarking can be used as a tool in KM especially for knowledge creation and
acquisition, but also for knowledge sharing phases of KM process. In the end, the value created by
benchmarking is still measured in the knowledge utilization phase. In all of these KM process phases there
can be several challenges for successful benchmarking. In this paper, the benefits and challenges of
benchmarking as a tool for KM is studied through two empirical, qualitative case studies from the Finnish
health care system. Empirical findings suggest that more effective benchmarking can be achieved by
strengthening strategy orientation and systematic approach. Strategy-driven benchmark practices ensure that
benchmarking is targeted correctly. In turn, systematic approach can be increased through well-planned
knowledge acquisition, sharing and documentation, and by harnessing operations in networks as a goal-
oriented part of the development of the health care organizations’ competencies and operations.
1 INTRODUCTION
Health care systems are one of the most critical
systems in societies (Keskimäki et al. 2019) and are a
solid foundation for the daily life of citizens.
Especially in the midst of crises, such as the COVID-
19 pandemics or wars which cause massive effects
around the world, resilience is required from
healthcare systems. The resilience of the health care
system can be seen in how quickly and at what
capacity health care can produce and provide health
care services to the entire community in the event of
a shock. (Lo Sardo et al., 2019) Knowledge
management (KM) has been identified as one of the
key factors in developing resilience (see e.g. Irfan et
al. 2022; Mafabi et al., 2013). The cornestones of KM
for development activities according to the work by
Sharma et al. (2013) can be listed as knowledge
creation; knowledge transfer and diffusion, and
knowledge utilisation and exploitation. As Sharma et
al. (2013) have stated, in many cases KM for
development activities requires benchmarks.
Benchmarking enables the process of acquiring and
transforming explicit and tacit knowledge (Massa &
Testa, 2004), which plays a central role in classic KM
models (Nonaka, 1994).
Benchmarking can be defined as the comparison
of strategies or processes within different industries;
finding best practices or benchmark can enhance
learning in the organisation (Grayson, 1992; Watson,
1994). Furthermore, benchmarking can prevent
unjustified complacency in an organisation, relying
on your own knowledge too much, for example
(Zairi, 1994) and it can also enhance problem solving
(Andersen and Moen, 1999). Thus it is no surprise
that an increasing need for benchmarking has been
identified in the public sector too (Raymond, 2008;
Hong et al., 2012). To succeed, benchmarking needs
management support, as a strategy-based
benchmarking process needs to be planned, organised
and managed besides requiring, understanding of the
organisation´s own processes before benchmarking
(Grayson, 1992). However, best practices are not
always transferable but may need modifications
because of the cultural context or sectoral legislation
(Watson, 1994).
Municipalities, including cities, often play a key
role in developing healthcare in societies. Thus, they
have huge responsibilities and face many challenges
in their development activities in the healthcare
context. In this paper, we aim to identify the benefits
and challenges of benchmarking in two cases from
Finland: a city organization involved in organizing
Paunu, A., Väyrynen, H. and Helander, N.
Knowledge Management and Benchmarking for Health Care System Development Activities.
DOI: 10.5220/0011540800003335
In Proceedings of the 14th International Joint Conference on Knowledge Discovery, Knowledge Engineering and Knowledge Management (IC3K 2022) - Volume 3: KMIS, pages 163-168
ISBN: 978-989-758-614-9; ISSN: 2184-3228
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
163
health care services and a Wellbeing services county
of Pirkanmaa.
The remain of the paper is organized as following.
Theoretical bases of benchmarking is first introduced.
Research method and the case organizations are then
briefly introduced and followed by the description of
the key results of the empirical study. The paper is
finalized by the conclusions and discussion section.
2 BENCHMARKING PROCESS
The benchmark process consists of many sources of
information, various actors and step-by-step phases of
different tasks. Benchmarking can target the
individual or team level, organizational level, urban,
regional or national level. (Spendolini, 1992) For
example, a single comparison can be made at city
level, with the aim of finding out how the city ranks
on a specific theme in a global-level comparison.
Another identifiable target could be the comparison
of the best practices regarding a product or process.
(Wolfram Cox et al., 1997) The tools of the
benchmarking process that are selected are also
influenced by whether the benchmarking is being
carried out to compare the organisation's own
practices or learning (Braadbaart and Yusnandarshah,
2008), strategy-level planning, strategic choices or
implementations (Chase, 1997), or to compare the
performance of the organisation against other
organisations (Kim and Lee, 2010). This paper
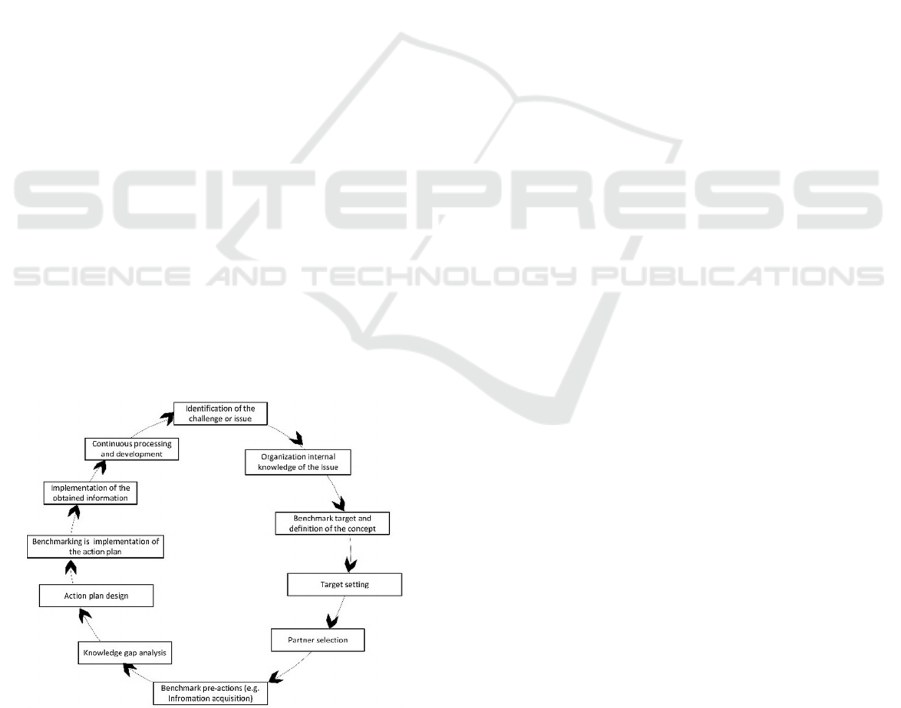
considers benchmarking through Anand and Kodali´s
benchmarking model (2008). The modified steps of
the benchmarking actions are introduced in Figure 1
below.
Figure 1: Benchmarking process steps (modified from
Anand and Kodali, 2008).
The benchmarking process begins by identifying the
topic, i.e. what kind of new and comparable
information is needed. There will be a lot of internal
tacit knowledge in the organisation, and it is worth
finding out about the organisation´s own knowledge
and expertise in the topic.
A more accurate definition of the benchmark is an
important step. Framing a topic with a specific
concept helps the benchmarkerkers in the data
acquisition process (e.g., Francis and Holloway,
2007). The point of comparison in the benchmarking
should also be limited, for example, regional
delimitation would targets the data acquisition source
material more precisely.
The setting of a target is important in order to
clarify the idea of the benchmarking objectives and to
have a common understanding of what one wants to
achieve (Watson, 1994). Target setting is also
important for assessing subsequently whether the
desired information was obtained and whether the
objectives set by the benchmarking were achieved.
Choosing a partner means, selecting a partner to
carry out the process itself or other collaborators.
Knowledge at the network level is multidimensional;,
partners share industry specific knowledge with
members of the network, as well as the organisation’s
internal knowledge (Sammarra and Biggiero, 2008)
Therefore, shared resources in implementation guide
the benhmarkers to focus on their own use of know-
how in the process itself. For example, external
organisations or research institutions may offer their
services to support the partial implementation (e.g.
literature review, interviews, etc.) or the process
implementation as a whole.
Before the actual visit the benchmarking terget, to
another city or country, benchmarking pre-work
includes the information acquisition process. There
are different search portals or databases for searching
for and analysing targeted information about
products, services or processes, e.g. case studies,
specific themes, cities or organisations that have been
made earlier (Castro and Frazzon, 2017). It is worth
formulating a few relevant benchmark questions with
the team is good to formulate in order to reflect on
and find answers to the benchmarking challenge or
issue in advance. Based on the benchmarking
material already found, a data gap analysis will reveal
what has already been studied on a particular topic
(and where).
The development of the benchmarking plan will
help to focus on the essential in the information
search: objectives for the benchmarking and how to
implement the benchmarking (e.g. visit, online
meeting, consultancy or database-based survey). It is
also a good idea to include, for example, the intended
contact persons, the scheduling of operations and the
KMIS 2022 - 14th International Conference on Knowledge Management and Information Systems
164

persons responsible for the different stages in the
process itself (Watson, 1994).
The benchmarking process also includes the
implementation of the action plan (Shiem-Shin Then,
1996), which needs to be flexible. For example, the
original contact persons may change to another
person who uses their own networks to lead the
process perhaps in a different direction than planned.
Otherwise, in this phase it is essential to keep in mind
the objectives of the benchmarking and the
benchmark questions, to which answers are being
sought. If a large group participates in a visit or
network meeting, sharing the research questions
among the group members will help to focus on
capturing the most relevant information from the
discussions. The obtained information can be
documented later.
The obtained benchmark information needs a
implementation plan as well (as part of the action
plan); what and how the information is to be shared
with a wider range of organisations, what information
is to be shared publicly, how the results can be
documented easily and quickly, and how to
implement the obtained experience in the
organisation's activities or whether pilots are to be
carried out (Feizabadi et al., 2019). After these
questions, the organisation will evaluate what was
learnt in the benchmarking process, and share the
lessons learned more widely with the public.
Simultaneously, the final stage of the benchmarking
process, continuous processing and the development
phase, will lead the organisation to consider how the
data on different issues can be utilised and how the
experiences gained from the compared objects can be
implemented in its own operations, strategic planning
or decision-making processes.
3 RESEARCH METHODS AND
CASE STUDY DESCRIPTION
The case studies focuses on a medium sized city
(referred to later in the text as City) in Finland. The
City has a key role in organizing the healthcare
services for the citizens in the municipal area in close
cooperation with other local and national level
authorities. In order to provide empirical insights of
the current situation of using benchmarking as a tool
for knowledge management and development
activities, semi-structured interviews and facilitated
workshops were organized in first case. The
participants represented the different service units
with various positions in the City’s organisations. A
total of 30 interviews were conducted from December
2020 to January 2021, recorded and transcribed
afterwards. The interviewees’ positions in the
organization’s hierarchy varied from coordinators
on the operational level to the upper management.
The interviews were analysed using content analysis.
The workshops were held in spring and autumn 2021.
The second case had six facilitated workshops in
autumn of 2021. The participants represented
different health care and rescue service units with
various positions in the organizations of the
municipalities in Pirkanmaa area. With total 55
participants of which some of the participants were
taking part of several workshops. During the
workshop the more detailed explanation of the results
was asked from the participants to get deeper
understanding of the benchmark activities in
Wellbeing services county of Pirkanmaa. In the
following section we introduce, how the
benchmarking concept was understood, how the
information was stored and knowledge shared as well
as the challenges and benefits of benchmarking
identified in the case studies.
4 CASE STUDY RESULTS
In the current situation, benchmark is understood as
learning from others, the exchange of best practices,
experiences and exchange of knowledge. The
important role of benchmarking was in the utilization,
evaluation and comparison of different issues
concerning the knowledge obtained. Benchmarking
enabled the own positioning of the City with
regarding to health care providers with different
actors, countries or cities.
Currently, benchmarking activities are carried out
in different service units. In some units,
benchmarking has become part of the work activities
and culture, while on the other hand, benchmarking is
not considered to be part of the work tasks at all in
some units, although there is pressure for change.
Benchmarking activities currently lack planning and
systematicity, and the emphasis is more on the
random and unstructured nature of benchmarking
operating management. The basis and objectives of
benchmarking are derived from the City's strategy
(especially in development projects, new services or
emphasized priorities); however, this needs more
active internal presentation and structuring.
Benchmarking activities do not appear as part of the
units’ annual planning, except large for scale projects,
in which case the needs for benchmarking are
comprehensively written down in the action plan (i.e.
Knowledge Management and Benchmarking for Health Care System Development Activities
165
what items need to be benchmarked, goal setting is
considered and scheduled and the implementation of
the results is planned).
The cases addressed the utilisation of benchmark
data and information, storage, sharing and
implementation in benchmark activities. Currently,
benchmarking information is not collected, stored or
shared systematically using any program or tool. The
information remains with the individual employee,
who thus accumulates large amounts of tacit
knowledge. Information storage is often in a private
computer or network folder, and access to the data is
limited. The means for result sharing are team
meetings or management teams. Currently, the
benchmark information and results are distributed
randomly, and there is no mutually agreed practice for
storing or sharing of benchmark information and
result. Therefore there was a wish to develop a wide
range of services provided by the organisation, such
as a handbook or model for making an impact on
benchmarking, a means of prior preparation, easy and
practical guidance, a way to implement
benchmarking, training in benchmarking, and also
practical assistance for the benchmarking process and
supporting materials for learning and utilization of
health care IT systems.
Empirical results highlighted increasing
understanding of benchmarking as such, and the fact
that benchmarking process enhanced their
understanding of the benchmarked issue. In
benchmarking, "there is no need to reinvent the
wheel", but benchmarking makes it easier to set the
scale, identify errors, gain objectivity and
phenomenon-based examination” said one of the
interviewees. Benchmark activities are often reflected
positively in the operating and work culture, creating
trust, openness and co-creation between different
actors in international cooperation.
The benefits of benchmarking identified in the
workshops, especially in the health care context
include learning from others and particularly, the
need to make tacit knowledge visible and shared.
Benchmarking offers a tool for forming the security
situational picture of the overall health and welfare
sector at the national level, for example (i.e. risk
evaluation or administration or leadership needs).
Beside learning and the situational picture,
benchmarking reveals the opportunities for co-
operation between different actors in a certain field.
Furthermore, technology is developing rapidly and
technological solutions in the health and wellbeing
sector require constant learning, and benchmarking
was seen as a tool for co-learning.
There are also challenges or obstacles to
benchmarking. Our results highlighted time,
competence and human resources as the challenges
faced in benchmarking. The network challenges
identified were different cultures, differences in
services and systems (i.e. Finnish social security,
education arrangements, etc.) and language issues.
However, the City's internal policies and rules (i.e.
travel rules) constrain benchmarking operations. The
identified challenges in health care become
emphasized in the transformation of the operational
environment; technology shapes the operational
environment and the learning requirements are
continuous: increasing customer needs lead to a more
and more to customer-oriented approach and different
experiences from other actors are needed for service
development. The participants emphasized the need
for support for evaluation, object definition and
vision formulation, and benchmarking is one tool for
these. The empirical results highlighted several
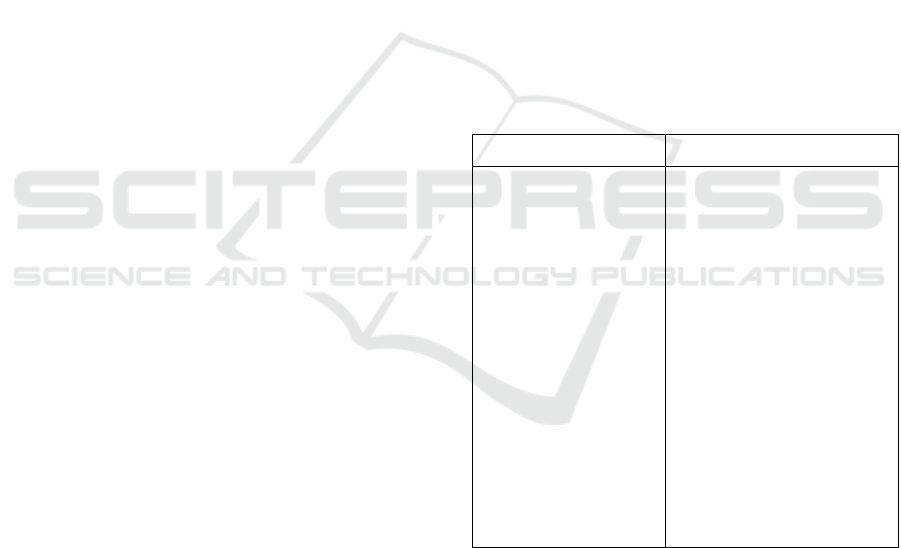
aspects of the benefits as well as challenges (Table 1).
Table 1: Identified benefits and challenges of
benchmarking in the case studies.
BENEFITS CHALLENGES
LEARN
Lessons learned,
expanding your own
understanding and
experiences, new
insights
ACT
Trust, cooperation,
internationality, set
scale for operations,
positioning
DEVELOP
New ideas, piloting, co-
creation, reflected in the
operating culture,
enhanced knowledge,
attitude change
RESOURCES
Lack of time for
benchmarking, implementing
new ideas random
INFORMATION
Person-linked tacit
knowledge, employee
turnover, documentation,
knowledge exchange and
sharing
CULTURE
System and cultural
differences, language issues,
comparability, alignment
with context
PROCEDURE
Bureaucracy, policy
5 CONCLUSIONS AND
DISCUSSION
At its best, benchmarking information should be of
high quality and easily accessible to support decision
makers. In order to ensure the functioning of this
chain, it is necessary to reconcile both the more
technical side (such as functioning information
systems to enable data storage) and the softer, more
KMIS 2022 - 14th International Conference on Knowledge Management and Information Systems
166

human side. One practical tool for information
processing could be the information management
process model developed by Choo (2002), which
begins with defining information needs and acquiring
information. The data analysis phase is when data
collected from different sources is analysed. The next
step in the process is information sharing and
utilisation. However, information will only become
valuable when it is used in decision-making and
operational development, and when real changes in
the organisation's operations take place. It is essential
to evaluate the changes through measuring and what
is learned from the benchmarking process. In that
way, by identifying new development needs, the
information management cycle starts again.
As in the benchmarking process, the information
process requires the selection of the theme and the
definition of the concept of the issue; what is actually
to be examined in benchmarking. The object setting
for benchmarking guides the benchmarkers and
potential data users to consider what is the desired
outcome as well as who will benefit from the results
and how.
The next step is to define the data source for data
acquisition and to define how the data source will be
analysed. Data can be retrieved using different
databases, and it is essential is to identify the most
relevant data for the benchmarking purpose. The
benchmark information obtained needs
implementation steps. The results gained in the
benchmark information process can guide
knowledge-based decision making.
In summary, more effective benchmarking can be
achieved by strengthening the strategy orientation
and systematic approach. Strategy-driven benchmark
practices ensure that benchmarking is targeted
correctly. In turn, a systematic approach can be
increased through systematic data collection, sharing
and documentation, and by harnessing operations in
networks as a goal-oriented part of the development
of the organisation's competence and operations.
Finally, the results obtained should mirror the
objectives set for the benchmarking (how the targets
were achieved or why they were not met).
This study has several limitations that affect
especially the generalizability of the research results.
The empirical data is gathered only from two cases,
both representing Finnish health care system, which
in turn is a representative of the so-called Nordic
health care system. Furthermore, empirical data was
gathered only by qualitative means, thus the study is
lacking quantitative evidence. However, this study
was able to provide initial empirical insights of the
benefits and challenges that health care service
organizations face in development activities. Further
empirical studies are needed, as well as more solid
analysis of the overall KM process and its relation to
benchmarking phases.
ACKNOWLEDGEMENTS
This work is a part of the RECPHEALS project,
funded by Academy of Finland, Special funding for
research into crisis preparedness and security of
supply.
REFERENCES
Anand, G. and Kodali, R., 2008. Benchmarking the
benchmarking models. Benchmarking: An
International Journal, Vol. 15(3), pp. 257-291.
doi.org/10.1108/14635770810876593.
Andersen, B. & Moen, R. 1999. Integrating benchmarking
and poor quality cost measurement for assisting the
quality management work. Benchmarking: An
International Journal, Vol. 6(4), pp. 291-301.
Bhutta, M., Huq, F. 1999. Benchmarking – Best Practices:
An Integrated Approach. Benchmarking: An
International Journal, Vol 6 (3), pp. 254-268.
Braadbaart, O. and Yusnandarshah, B. 2008, Public sector
benchmarking: a survey of scientific articles, 1990-
2005, International Review of Administrative Sciences,
Vol. 74(3), pp. 421-433.
Castro, V. & Frazzon, E.M., 2017. Benchmarking of best
practices: an overview of the academic literature.
Benchmarking: An International Journal, Vol. 24(3),
pp. 750-774. https://doi.org/10.1108/BIJ-03-2016-0031.
Chase, R. L. 1997. Knowledge Management
Benchmarks. The Journal of Knowledge Management,
Vol.1(1), pp. 83-92.
Choo, C.W. 2002. Information management for the
intelligent organization: the art of scanning the
environment. Medford, New Jersey, Information
Today, Inc.
Feizabadi, J., Maloni, M. and Gligor, D., 2019.
Benchmarking the triple-A supply chain: orchestrating
agility, adaptability, and alignment. Benchmarking: An
International Journal, Vol. 26 (1), pp. 271-295.
https://doi.org/10.1108/BIJ-03-2018-0059.
Francis, G. & Holloway, J. 2007. What have we learned?
Themes from the literature on best-practice
benchmarking. International Journal of Management
Reviews, 9(3), pp. 171-189. doi.org/10.1111/j.1468-
2370.2007.00204.x.
Grayson, C. J. Jr. 1992. Taking on the world. The TQM
Magazine, Vol. 4(3), pp. 139-142. doi.org/10.1108
/09544789210034365
Hong, P., Hong, S.W., Roh, J.J. and Park, K. 2012.
Evolving benchmarking practices: a review for research
Knowledge Management and Benchmarking for Health Care System Development Activities
167

perspectives, Benchmarking: An International Journal,
Vol. 19(4/5), pp. 444-462.
Irfan, I., Sumbal, M.S.U.K., Khurshid, F. and Chan, F.T.S.
2022. Toward a resilient supply chain model: critical
role of knowledge management and dynamic
capabilities. Industrial Management & Data Systems,
Vol. 122(5), pp. 1153-1182. doi.org/10.1108/IMDS-
06-2021-0356
Keskimäki, I., Tynkkynen, L.-K., Reissell, E. et al. 2019.
Finland: health system review. World Health
Organization. Regional Office for Europe, European
Observatory on Health Systems and Policies.
Kim, S. & Lee, H. 2010. Factors affecting employee
knowledge acquisition and application capabilities.
Asia-Pacific Journal of Business
Administration, Vol. 2(2), pp. 133-152.
Lo Sardo, D.R., Thurner, S., Sorger, J., Duftschmid, G.,
Endel, G., Klimek, P. 2019. Quantification of the
resilience of primary care networks by stress testing the
health care system. Proceedings of the National
Academy of Sciences of the United States of America.
doi.org/10.1073/pnas.1904826116. 2019.
Mafabi, S., Munene, J. C., & Ahiauzu, A. 2013.
Organisational resilience: Testing the interaction effect
of knowledge management and creative climate.
Journal of Organizational Psychology, 13(1/2), pp. 70-
82.
Massa, S., & Testa, S. 2004. Innovation or imitation?
Benchmarking: a knowledge‐management process to
innovate services. Benchmarking: An International
Journal, Vol. 11(6), pp. 610-620. doi.org/10.1108/
14635770410566519
Nonaka, I (1994) A dynamic theory of organizational
knowledge creation. Organization Science 5(1), pp. 14–
37.
Raymond, J. 2008. Benchmarking in public procurement,
Benchmarking: An International
Journal, Vol. 15(6), pp. 782-793.
Sammarra, A. and Biggiero, L. 2008. Heterogeneity and
specificity of inter-firm knowledge flows in innovation
networks, Journal of Management Studies, Vol. 45(4),
pp. 800-829.
Sharma, R. S., Iqbal, M. I. N. A., & Victoriano, M. M. 2013.
On the use of benchmarking and good practices for
knowledge management for development. Knowledge
Management Research & Practice, 11(4), 346-360.
Shiem‐Shin Then, D. 1996. Minimum data sets ‐ finding
the balance in benchmarking. Facilities, Vol. 14(1/2),
pp. 47-51. doi.org/10.1108/02632779610108495
Spendolini MJ., 1992. The Benchmarking Process.
Compensation & Benefits Review, 24(5), pp. 21-29.
doi:10.1177/088636879202400505.
Watson, G. H. 1994. A Perspective on Benchmarking.
Benchmarking for Quality
Management & Technology, Vol. 1(1), pp. 5-10.
Wolfram Cox, J.R., Mann, L. & Samson, D. 1997.
Benchmarking as a Mixed Metaphor: Disentangling
Assumptions of Competition and Collaboration.
Journal of Management Studies, 34, 285-314.
doi.org/10.1111/1467-6486.00052.
Zairi, M. 1994
. Benchmarking: The Best Tool for
Measuring Competitiveness. Benchmarking for
Quality Management & Technology, Vol. 1(1), pp. 11-
24.
KMIS 2022 - 14th International Conference on Knowledge Management and Information Systems
168
