
Undiagnosed Hypertension and Associated Factors among Adults in
Kalimantan, Indonesia
Ayunina Rizky Ferdina
1
and Arief Budiman
2
1
Research Center for Public Health and Nutrition, National Research and Innovation Agency, Bogor, Indonesia
2
Department of Health Information Management, Health Polytechnic Kesdam VI, Banjarmasin, Indonesia
Keywords: Undiagnosed Hypertension, Risk Factors, Lifestyle, Sociodemographic, Blood Pressure.
Abstract: Hypertension prevalence in Kalimantan is relatively high compared to in other Indonesian regions but most
of the cases were undiagnosed. This study aimed to determine the prevalence of undiagnosed hypertension
and analyze the related sociodemographic and lifestyle factors among adults in Kalimantan, Indonesia. An
observational, cross-sectional study was performed using data from Riskesdas 2018. Undiagnosed
hypertension is operationally defined as having systolic blood pressure > 140 mmHg and/or diastolic blood
pressure > 90 mmHg in the blood pressure measurement conducted in the Riskesdas survey, with no prior
diagnosis of hypertension by any health care professional. Odds ratios (OR) computed by logistic regression
were estimated to determine the factors associated with undiagnosed hypertension. The undiagnosed
hypertension in this population was more prevalent and had significant differences (p < 0.001) among those
who are below 30 years old, living in rural areas, as well as those consuming fruits and/or vegetables > 5
portions/day. Certain characteristics revealed in this study as having significant associations with undiagnosed
hypertension may be used as guidance in prioritizing hypertension screening in Kalimantan. .
1 INTRODUCTION
Increased blood pressure can trigger various kinds of
non-communicable diseases (Kalehoff & Oparil,
2020). It is one of the main causes of premature death
in the world. Since a portion of those who exhibit this
clinical condition are unaware of it, hypertension is
often called the "silent killer" (World Health
Organisation (WHO), 2013). A delayed diagnosis of
hypertension may cause increased cardiovascular
risks (Forouzanfar et al., 2017).
It is already obvious that the trend of hypertension
is increasing all over the world, including in
Indonesia (Purnamasari, 2018). The prevalence of
hypertension is especially high in Kalimantan, which
is the Indonesian part of Borneo Island. Almost all of
the Kalimantan provinces have hypertension cases
above the national level based on the blood pressure
measurement data from the latest Indonesian Basic
Health Research (Riskesdas, acronym in Indonesian)
(Ministry of Health of Indonesia, 2018a, 2018b).
However, most of the hypertension cases in this
Indonesian part of Borneo Island were not diagnosed
by health professionals prior to the survey (Ministry
of Health of Indonesia, 2018b).
It shows that Kalimantan faces a challenge to
increase awareness of hypertension among its
citizens. Without awareness, it is difficult to get
individuals to seek treatment and modify their
lifestyle to control their blood pressure. A study from
another Asian country reported that undiagnosed
hypertension poses a serious threat to the
development of cardiovascular disease, chronic
kidney disease, and all-cause mortality (Choo et al.,
2014).
To our knowledge, study on undiagnosed
hypertension is still lacking in this biggest island of
the country. Therefore, this study examined whether
individuals who were unaware of their hypertension
condition differed from those who have been
diagnosed with the disease. We aimed to assess the
prevalence of undiagnosed hypertension among
adults in Kalimantan and analyze the associated
factors, which would include sociodemographic and
lifestyle factors.
154
Ferdina, A. and Budiman, A.
Undiagnosed Hypertension and Associated Factors among Adults in Kalimantan, Indonesia.
DOI: 10.5220/0011650700003608
In Proceedings of the 4th International Conference on Social Determinants of Health (ICSDH 2022), pages 154-160
ISBN: 978-989-758-621-7; ISSN: 2975-8297
Copyright
c
2023 by SCITEPRESS – Science and Technology Publications, Lda. Under CC license (CC BY-NC-ND 4.0)

2 METHODS
2.1 Study Design
This is an observational, cross-sectional study using a
database of Riskesdas 2018. Riskesdas is a
nationwide survey directed by the Ministry of Health
of Indonesia and the detailed protocol can be found in
its final report (Ministry of Health of Indonesia,
2018b). Riskesdas 2018 samples were selected
through a two-stage stratified cluster sample drawn
from across the nation.
2.2 Sample
In this study, the population of interest was only those
residing in Kalimantan, Indonesia. Besides that, the
inclusion criteria include age over 18 years old,
located in Kalimantan, not pregnant, and having
blood pressure data from the survey. This led to a
dataset containing 35,991 adult subjects who were
Riskesdas 2018 respondents from Kalimantan whose
blood pressure data were collected. We then selected
7,908 hypertensive individuals that were determined
referring to their blood pressure data to be analyzed.
2.3 Variables
The dependent variable was the presence of
hypertension diagnosis prior to the survey,
constructed from the survey data. Undiagnosed
hypertension was defined if, at the time of the survey,
a subject had a mean SBP value > 140 mmHg and/or
a mean DBP > 90 mmHg blood pressure data
compatible with hypertension in the two blood
pressure measurements and that hypertension had not
been previously diagnosed by any health
professional. Otherwise, it was defined as diagnosed
hypertension.
The independent variables consist of several
sociodemographic and lifestyle characteristics. The
sociodemographic characteristics include age group,
gender, area of residence, occupation, and
educational level. Lifestyle characteristics that are
used as the independent variables include behaviors
on smoking, alcohol consumption, physical activity,
as well as consumption of some food categories.
Physical activities are categorized into “active” and
“inactive” based on the modified Global Physical
Activity Questionnaire which is part of the WHO
STEPS instrument (Ministry of Health of Indonesia,
2018b).
Simple questionnaires and food cards were used
to ask about the consumption frequency of several
food groups, including salty foods, preserved meat,
instant foods, and instant seasonings. The frequency
of consuming such foods was categorized into “daily”
and “not daily”. The frequency of fruit and vegetable
consumption was also asked and then categorized into
>5 portions/day and < 5 potions/day. All of those data
were collected using a validated questionnaire
delivered by trained enumerators (Ministry of Health
of Indonesia, 2018b).
2.4 Ethical Consideration
For the primary data collection of Riskesdas 2018, the
Ethical Committee of Health Research, NIHRD,
Ministry of Health of Indonesia had given their
approval with the reference number
LB.02.01/2/KE.267/2017. Secondary analysis of the
obtained data requires no additional ethical clearance.
2.5 Statistical Analysis
Univariate analyses were performed to characterize
the study population. Bivariate analyses were
conducted to compare the prevalence of diagnosed
and undiagnosed hypertension as well as to obtain
crude odds ratio (OR) together with their 95%
confidence intervals (CI). Subsequently, with the
factors which obtained a value of p < 0.20, a
multivariate regression model was estimated to obtain
adjusted odds ratios (aOR) together with their 95%
CI. Significance is determined at p < 0.05. A complex
sample technique was employed in all analyses, that
were performed using the International Business
Machines Statistical Package for the Social Sciences
(IBM SPSS) version 25.
3 RESULTS
We analyzed almost eight thousand subjects located
in Kalimantan who had hypertension during
Riskesdas 2018 survey. The distribution of our study
subjects disaggregated by their diagnosis status for
hypertension and independent variables is described
in Table 1.
Undiagnosed Hypertension and Associated Factors among Adults in Kalimantan, Indonesia
155

Table 1: Description of subjects’ characteristics and
their diagnosis status of hypertension.
Characteristic N
H
ypertension diagnosis status
Diagnosed
% (95% CI)
Undiagnosed
% (95% CI)
Age group (years)
19-29 399 57.1(49.4-64.5) 42.9(35.5-50.6)
30-39 1018 67.3
(
63.3-71
)
32.7
(
29-36.7
)
40-49 2252 75.7
(
73.2-78
)
24.3
(
22-26.8
)
50-59 2274 80
(
77.7-82.1
)
20
(
17.9-22.3
)
60 or more 1965 80.2(77.8-82.4) 19.8(17.6-22.2)
Gende
r
Male 3071 73.4
(
71.1-75.6
)
26.6
(
24.4-28.9
)
Female 4837 77.7
(
76.1-79.3
)
22.3
(
20.7-23.9
)
A
rea of residence
Urban 3889 79.4
(
77.4-81.3
)
20.6
(
18.7-22.6
)
Rural 4019 72.8(70.9-74.6) 27.2(25.4-29.1)
Employment status
Formal employee 1076 75.6(71.9-79) 24.4(21-28.1)
Entre
p
reneu
r
1203 76.1
(
72.7-79.2
)
23.9
(
20.8-27.3
)
Farmer/fisherman 1839 71.2
(
68.4-73.8
)
28.8
(
26.2-31.6
)
Informal worke
r
915 75.5
(
71.4-79.2
)
24.5
(
20.8-28.6
)
In school/not
employe
d
2875 79.5(77.4-81.4) 20.5(18.6-22.6)
Educational level
Graduated high
school
2247 77.3(74.6-79.7) 22.7(20.3-25.4)
Never graduated
hi
g
h school
5661 75.6(74-77.1) 24.4(22.9-26)
Smoke
r
Yes, dail
y
1552 72.1(69-75) 27.9(25-31)
Yes, not dail
y
629 72.8(67.1-77.8) 27.2(22.2-32.9)
Neve
r
5727 77.5
(
75.9-79
)
22.5
(
21-24.1
)
Alcohol drinke
r
Yes 198 69.5
(
61.2-76.7
)
30.5
(
23.3-38.8
)
No 7710 76.2(74.8-77.6) 23.8(22.4-25.2)
Physical activit
y
Active 5335 74.8(73.2-76.4) 25.2(23.6-26.8)
Inactive 2573 78.6
(
76.3-80.6
)
21.4
(
19.4-23.7
)
Food consumption
Vegetable
> 5 portions/day 5592
76.9
(
75.3-78.4
)
23.1
(
21.6-24.7
)
< 5 portions/day 2316
74.1
(
71.5-76.5
)
25.9
(
23.5-28.5
)
Fruit
> 5 portions/da
y
1609 80.8(78-83.2) 19.2(16.8-22)
< 5
p
ortions/da
y
6299 74.8
(
73.3-76.4
)
25.2
(
23.6-26.7
)
Salt
y
foo
d
Dail
y
1544 75.3
(
72-78.2
)
24.7
(
21.8-28
)
Not dail
y
6364 76.2(74.7-77.7) 23.8(22.3-25.3)
Instant foo
d
Dail
y
557 75.2(70.1-79.6) 24.8(20.4-29.9)
Not dail
y
7351 76.1
(
74.7-77.5
)
23.9
(
22.5-25.3
)
Preserved meat
Dail
y
209 80.7
(
72.2-87
)
19.3
(
13-27.8
)
Not dail
y
7699 75.9(74.5-77.2) 24.1(22.7-25.5)
Seasoning
Dail
y
5773 76
(
74.4-77.5
)
24
(
22.5-25.6
)
Not dail
y
2135 76.1
(
73.6-78.5
)
23.9
(
21.5-26.4
)
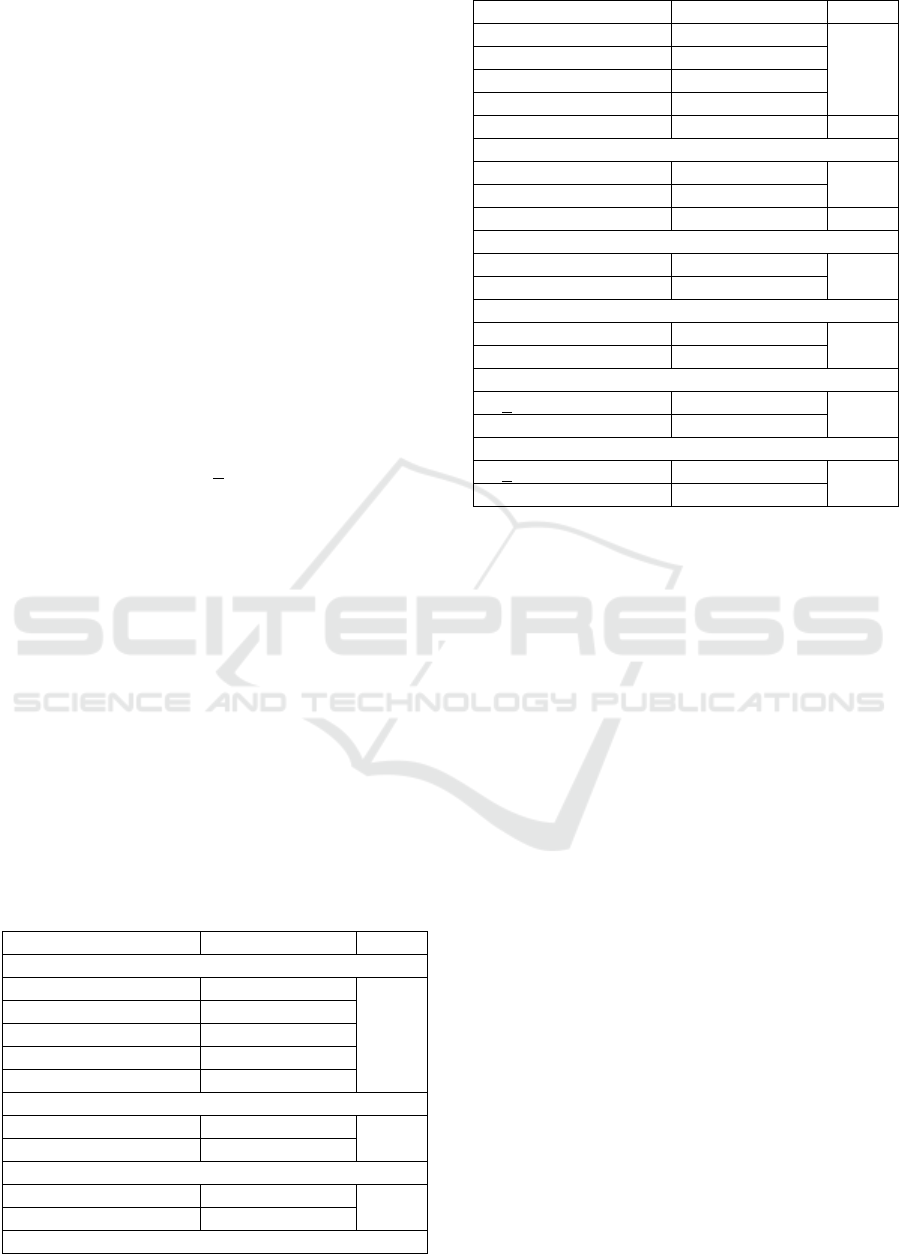
Table 2: Bivariate analysis between respondents'
characteristics and undiagnosed hypertension.
Characteristics Odds Ratio P
Age group (years)
19-29 Ref
< 0.001
30-39 0.649(0.457-0.923)
40-49 0.428 (0.304-0.603)
50-59 0.333 (0.238-0.467)
60 or more 0.328 (0.234-0.461)
Gender
Male 1.262 (1.099-1.451)
0.001
Female Ref
Area of residence
Urban 0.694 (0.596-0.809)
< 0.001
Rural Ref
Employment status
Formal employee 1.248 (0.996-1.565)
< 0.001
Entrepreneur 1.217 (0.978-1.513)
Farmer/fisherman 1.569 (1.319-1.867)
Informal worker 1.253 (0.987-1.59)
In school/not employed Ref
Educational level
Graduated high school Ref
0.260
Never graduated high
school
1.099 (0.932-1.296)
Smoke
r
Yes, dail
y
1.334 (1.129-1.576)
0.003
Yes, not dail
y
1.286 (0.972-1.702)
Neve
r
Ref
Alcohol drinke
r
Yes 1.403 (0.968-2.033)
0.072
No Ref
Physical activit
y
Active Ref
0.006
Inactive 0.812 (0.699-0.942)
Food consumption
Vegetable
> 5 portions/da
y
Ref
0.046
< 5
p
ortions/da
y
1.164 (1.002-1.351)
Fruit
> 5 portions/da
y
Ref
<
0.001
< 5 portions/da
y
1.41 (1.17-1.699)
Salty foo
d
Dail
y
1.055 (0.877-1.269)
0.571
Not dail
y
Ref
Instant foo
d
Dail
y
1.053 (0.804-1.379)
0.707
Not dail
y
Ref
Preserved meat
Dail
y
0.755
(
0.467-1.219
)
0.249
Not dail
y
Ref
Seasoning
Daily 1.007 (0.861-1.177)
0.933
Not daily Ref
ICSDH 2022 - The International Conference on Social Determinants of Health
156
The majority of the hypertensive subjects in this study
were between the age range of 50-59, female, not
employed, and never graduated high school. Most of
them are physically active and consume neither
cigarettes nor alcohol. Their proportions based on the
type of residency were almost the same between
urban and rural. In contrast to fruit consumption,
more than half of our subjects consume vegetables in
at least 5 portions daily.
We found that almost a quarter (24%; 95%CI
22.6-25.3%) of the subjects had no prior diagnosis
regarding their hypertension status. The prevalence of
undiagnosed hypertension in this population is the
highest among young adults and the lowest among the
elderly. Undiagnosed hypertension is also more
prevalent among those who never graduated high
school, live in a rural area, are males, and work as
farmers or fishermen (Table 1).
Except for educational level, the analyzed
sociodemographic characteristics showed statistically
significant associations (p < 0.001) with the diagnosis
status of hypertension (Table 2). Educational level is
also the only sociodemographic variable that was not
included in the multivariate analysis since the p is
higher than 0.2. Meanwhile, for lifestyle aspects, only
the status of smoker and alcohol drinker, physical
activity, as well as fruit and vegetable consumption
were included in the multivariate analysis.
In the final model, it was found that age group,
area of residence, fruit and vegetable consumption are
the factors with significant associations with
undiagnosed hypertension. Being older than 59 years
has an odds ratio almost three times lower to get
undiagnosed hypertension. Living in a rural area
lowered the chance of having hypertension cases
undiagnosed. Meanwhile, lower consumption of fruit
and vegetable gave about a 20% increase in odds
ratios for undiagnosed hypertension (Table 3).
Table 3: Multivariate analysis between respondents'
characteristics and undiagnosed hypertension.
Characteristics aOR (95% CI) P
Age group (years)
19-29 Ref
< 0.001
30-39 0.613 (0.43-0.873)
40-49 0.414 (0.292-0.586)
50-59 0.318 (0.226-0.448)
60 or more 0.312 (0.221-0.441)
Gender
Male 1.11 (0.913-1.35)
0.294
Female Ref
Area of residence
Urban 0.754 (0.64-0.89)
0.001
Rural Ref
Employment status
Characteristics aOR (95% CI) P
Formal employee 1.087 (0.846-1.395)
0.055
Entrepreneur 1.096 (0.866-1.387)
Farmer/fisherman 1.333 (1.101-1.613)
Informal worker 1.151 (0.901-1.471)
In school/not employed Ref
Smoker
Yes, daily 1.194 (0.966-1.476)
0.198
Yes, not daily 1.212 (0.901-1.63)
Never Ref
Alcohol drinker
Yes 0.959 (0.662-1.389)
0.826
No Ref
Physical activity
Active Ref
0.17
Inactive 0.896 (0.766-1.048)
Vegetable
> 5 portions/day Ref
0.035
< 5 portions/day 1.177 (1.012-1.37)
Fruit
> 5 portions/day Ref
0.03
< 5 portions/day 1.239 (1.021-1.503)
4 DISCUSSIONS
This study pursued to determine the prevalence and
factors associated with undiagnosed hypertension
among adults in Kalimantan, Indonesia. The
prevalence of undiagnosed hypertension in low-and-
middle-income countries ranges between 12-50%
(Guerrero-díaz et al., 2021). Based on our analysis of
secondary data from Riskesdas 2018, almost a quarter
of the hypertension cases among adults in Kalimantan
were undiagnosed (Table 2).
In Riskesdas, the data about hypertension is
collected by measuring blood pressure and
additionally, by interviewing the subject about
whether or not they had been diagnosed with
hypertension or taking blood pressure lowering
medication. For all the five Indonesian provinces in
Kalimantan, the differences between those two types
of data are quite remarkable. The blood pressure
measurement showed that only North Kalimantan had
hypertension prevalence below the national level
(Ministry of Health of Indonesia, 2018b).
Nevertheless, the data showed that this newest
province of Kalimantan has around 30% of
hypertension among its population aged 15 and over.
Overall, 1 in 3 people in Kalimantan had a blood
pressure compatible with hypertension when
surveyed in Riskesdas 2018 (Ministry of Health of
Indonesia, 2018b). The high prevalence of
hypertension in Kalimantan has been a persistent
Undiagnosed Hypertension and Associated Factors among Adults in Kalimantan, Indonesia
157

trend at least since Riskesdas 2007 when South
Kalimantan once more became the province with the
highest prevalence of hypertension in the country
(Ministry of Health of Indonesia, 2007).
However, the numbers are not as high if we look
at the data on hypertension based on diagnosis
history. We could only find about 10% of this same
population who have been diagnosed as having
hypertension (Ministry of Health of Indonesia,
2018b). In other words, most people who have
hypertension were never been told by any health
professional regarding their blood pressure condition.
The prevalence of hypertension in Indonesia had
been reported by other researchers to increase with
age (Rahajeng & Tuminah, 2009). When we
disaggregated the data, we could see that the trend of
undiagnosed hypertension in Kalimantan seems to
decrease with age (Table 2). This contradicts the
general trend of hypertension, where older age is
known as a risk factor for high blood pressure
(Vokonas et al., 1988). Nevertheless, this makes
sense because at a young age, hypertension is usually
still at the early stage and asymptomatic. No wonder
people belonging to this age group do not likely to
feel the need to check their blood pressure (Johnson
et al., 2016). This may cause their hypertension to be
uncontrollable because of the lack of awareness
(Gooding et al., 2014).
Additionally, while hypertension in Indonesia has
been known to be more prevalent in urban areas
(Peltzer & Pengpid, 2018), our study showed that
undiagnosed cases were more common in rural area.
Awareness, treatment, and control of hypertension
were reported to be higher in urban communities than
in rural communities in low-and-middle-income
countries (Chow et al., 2013). This could be reasoned
by the limited availability of health care facilities and
probably some geographical barriers the access to
those facilities. To reach people with the least access
to healthcare facilities, we advised deploying more
healthcare professionals to the areas.
We also found that farmers and fishermen,
followed by other informal workers, are less likely to
know if they had high blood pressure. On the other
hand, those who are not employed or in school are
more likely to get a medical diagnosis when they have
hypertension. This is probably because those
agricultural workers are usually located in areas with
less access to healthcare. In the United States,
agricultural workers have been reported to be at
greater risk for poor access to healthcare (Hoerster et
al., 2011). Moreover, the informal workers usually
have lower educational attainment and our results
show that those who never graduated high school got
a higher chance of getting undiagnosed hypertension,
although the relationship is not statistically
significant. A similar result about the relationship
between educational level and undiagnosed
hypertension had been found in a study on the
Peruvian population (Guerrero-díaz et al., 2021). On
the other hand, analysis of Indonesian Family Life
Survey data showed that on the national level, higher
education might reduce the chance of undiagnosed
hypertension (Mahwati et al., 2022).
Gender is the only sociodemographic variable
showing a similar trend with hypertension regardless
of the diagnostic status, where the proportion of males
with hypertension is higher than that of females
(Gillis & Sullivan, 2016). Analysis of Riskesdas 2007
data reported that male has a higher risk of having
high blood pressure (Rahajeng & Tuminah, 2009).
The higher probability of having undiagnosed
hypertension in men could be explained by their
lower awareness of hypertension (Guerrero-díaz et
al., 2021). In our study, we found that undiagnosed
hypertension in Kalimantan is also more common
among men than women. However, the relationship
is not deemed statistically significant when it is
analyzed in the multivariate logistic regression.
We found several lifestyle aspects to be
associated with the difference in the prevalence of
undiagnosed hypertension. However, consumption of
risky food items that we analyzed here, was not found
to be associated with undiagnosed hypertension
(Table 2). Frequent consumption of salty foods,
instant foods, preserved meat, and seasonings may
influence the risk of having high blood pressure, at
least theoretically. Nevertheless, our results show that
the diagnosis status of hypertension is unrelated to the
consumption behavior of such foods. Likewise, the
status of being an alcohol drinker is also not related
to undiagnosed hypertension.
It has been established that fruit and vegetable
intake provides protective effects against
hypertension (Pienovi et al., 2015). Our results show
that undiagnosed hypertension is significantly more
prevalent among subjects consuming lesser amounts
of these fiber-rich foods. This is not supposed to
explain causation, but this may imply that when
people are aware of their hypertension after receiving
the medical diagnosis, they are more willing to eat
sufficient amounts of fruits and vegetables.
From other perspectives, it is also possible that
people diagnosed with hypertension were more
willing to adopt healthy behaviors than their peers
who have the same condition but never received the
diagnosis. This may explain why among our subjects,
the proportion of people who consume fruits and
ICSDH 2022 - The International Conference on Social Determinants of Health
158

vegetables abundantly is bigger among those with
diagnosed hypertension. Individuals with diagnosed
hypertension are more likely to quit smoking and
those at a younger age at diagnosis tended to work out
regularly (Kim & Andrade, 2019).
Some community health centers (Puskesmas) in
Kalimantan have area coverage that is too vast,
causing some residents to live too far from the closest
Puskesmas (Nisa et al., 2017). That may explain why
a significant proportion of the population neglect to
frequently check their health, particularly their blood
pressure. In communities with these features of geo-
locality, programs that promote early identification
and treatment of hypertension are required to
recognize and decrease the number of untreated
patients.
Better tracking of blood pressure levels, raising
awareness of the benefit of hypertension control, and
promoting healthy behavioral modification can all
improve health outcomes (Kim & Andrade, 2019).
This can be accomplished by encouraging routine
visits to medical care providers, providing
information about recommended lifestyle choices,
and better health monitoring.
Given the high prevalence of undiagnosed
hypertension, governments in Kalimantan need to
reinforce the prevention and control of high blood
pressure in the community, especially by increasing
the coverage of early detection since it can promote
public health (Choo et al., 2014). For Kalimantan, it
is recommended to prioritize the screening to those
who are young adults, living in a rural area, have low
educational levels, and are informal/agricultural
workers; since undiagnosed hypertension is more
common among those populations. In the meantime,
efforts to increase fruit and vegetable intake are also
suggested because undiagnosed hypertension is more
common among those with low consumption of these
food groups.
The main limitation of this study is being
observational and cross-sectional due to the nature of
Riskesdas data, thus precluding causal inferences.
The self-reported data in Riskesdas is also another
weakness of this study, where they are subject to bias
due to under-reporting and measurement error.
Nevertheless, this study provides some insights that
can be considered in organizing public health
attempts to reduce hypertension cases in Kalimantan.
5 CONCLUSIONS
These findings imply that a remarkable proportion of
hypertension cases in Kalimantan are undiagnosed.
The lack of awareness about blood pressure status
suggests that there should be more efforts to
strengthen for detecting undiagnosed hypertension.
Such screening should be prioritized for those more
vulnerable to undiagnosed hypertension, such as
young adults and rural residents. Our results also
indicate that without knowing their hypertension
status, people might less likely to consume sufficient
amounts of fruits and vegetables. Having a proper
diagnosis of hypertension may not only help people
to receive treatment but also control their blood
pressure by adopting a healthy lifestyle.
REFERENCES
Choo, E. H., Ihm, S. H., Lim, S., Chang, K., & Seung, K.
B. (2014). A simple screening score for undiagnosed
hypertension. International Journal of Cardiology, 172
(3), e465–e467. https://doi.org/10.1016/j.ijcard.2014.01.
040
Chow, C. K., Teo, K. K., Rangarajan, S., Islam, S., Gupta,
R., Avezum, A., Bahonar, A., Chifamba, J., Dagenais,
G., Diaz, R., Kazmi, K., Lanas, F., Wei, L., Lopez-
Jaramillo, P., Fanghong, L., Ismail, N. H., Puoane, T.,
Rosengren, A., Szuba, A., … investigators, P.
(Prospective U.R.E.S. (2013). Prevalence, Awareness,
Treatment, and Control of Hypertension in Rural and
Urban Communities in High-, Middle-, and Low-
Income Countries. JAMA, 310(9), 959–968.
https://doi.org/10.1001/jama.2013.184182
Forouzanfar, M. H., Liu, P., Roth, G. A., Ng, M., Biryukov,
S., Marczak, L., Alexander, L., Estep, K., Hassen
Abate, K., Akinyemiju, T. F., Ali, R., Alvis-Guzman,
N., Azzopardi, P., Banerjee, A., Bärnighausen, T.,
Basu, A., Bekele, T., Bennett, D. A., Biadgilign, S., …
Murray, C. J. L. (2017). Global Burden of Hypertension
and Systolic Blood Pressure of at Least 110 to 115 mm
Hg, 1990-2015. JAMA, 317(2), 165–182. https://
doi.org/10.1001/jama.2016.19043
Gillis, E. E., & Sullivan, J. C. (2016). Sex Differences in
Hypertension. Hypertension, 68(6), 1322–1327. https://
doi.org/10.1161/hypertensionaha.116.06602
Gooding, H. C., McGinty, S., Richmond, T. K., Gillman,
M. W., & Field, A. E. (2014). Hypertension awareness
and control among young adults in the National
Longitudinal Study of Adolescent Health. Journal of
General Internal Medicine, 29(8), 1098–1104. https://
doi.org/10.1007/s11606-014-2809-x
Guerrero-díaz, D. V., Hern, A., Montoya-rivera, W. C.,
Rojas-roque, C., & Alberto, M. (2021). Heliyon
Undiagnosed hypertension in Peru : analysis of
associated factors and socioeconomic inequalities ,
2019. 7(July). https://doi.org/10.1016/j.heliyon.2021.e
07516
Hoerster, K. D., Mayer, J. A., Gabbard, S., Kronick, R. G.,
Roesch, S. C., Malcarne, V. L., & Zuniga, M. L. (2011).
Impact of individual-, environmental-, and policy-level
Undiagnosed Hypertension and Associated Factors among Adults in Kalimantan, Indonesia
159

factors on health care utilization among US
farmworkers. American Journal of Public Health,
101(4), 685–692. https://doi.org/10.2105/AJPH.2009.
190892
Johnson, H. M., Warner, R. C., Lamantia, J. N., & Bowers,
B. J. (2016). “I have to live like I’m old.” Young adults’
perspectives on managing hypertension: A multi-center
qualitative study. BMC Family Practice, 17(1), 1–9.
https://doi.org/10.1186/s12875-016-0428-9
Kalehoff, J. P., & Oparil, S. (2020). The Story of the Silent
Killer : A History of Hypertension: Its Discovery,
Diagnosis, Treatment, and Debates. Current
Hypertension Reports, 22(9), 72. https://doi.org/
10.1007/s11906-020-01077-7
Kim, H., & Andrade, F. C. D. (2019). Diagnostic status and
age at diagnosis of hypertension on adherence to
lifestyle recommendations. Preventive Medicine
Reports, 13(November 2018), 52–56. https://doi.org/
10.1016/j.pmedr.2018.11.005
Mahwati, Y., Nurrika, D., & Latief, K. (2022). The
Determinants of Undiagnosed Hypertension Among
Indonesian Adults: A Cross-sectional Study Based on the
2014-2015 Indonesia Family Life Survey. Journal of
Preventive Medicine and Public Health, 55(1), 60–67.
https://doi.org/10.3961/JPMPH.21.500
Ministry of Health of Indonesia. (2007). Laporan Nasional
Riskesdas 2007. In Laporan Nasional 2007.
http://kesga.kemkes.go.id/images/pedoman/Riskesdas
2007 Nasional.pdf
Ministry of Health of Indonesia. (2018a). Hasil Utama
Riset Kesehatan Dasar (RISKESDAS) 2018.
https://doi.org/10.1088/1751-8113/44/8/085201
Ministry of Health of Indonesia. (2018b). Laporan
Nasional Riskesdas 2018.
Nisa, L. S., Siska, D., Maliani, Putryanda, Y., Noor, G. S.,
& Wajidi. (2017). Pemetaan Fasilitas Kesehatan pada
Puskesmas di Kalimantan Selatan. Jurnal Kebijakan
Pembangunan, 12(2), 219–229.
Peltzer, K., & Pengpid, S. (2018). The Prevalence and
Social Determinants of Hypertension among Adults in
Indonesia: A Cross-Sectional Population-Based
National Survey. https://doi.org/10.1155/2018/56107
25
Pienovi, L., Lara, M., Bustos, P., & Amigo, H. (2015).
Consumo de frutas, verduras y presión arterial. Un
estudio poblacional [Fruit and vegetable intake, and
blood pressure. A population research]. Archivos
latinoamericanos de nutricion, 65(1), 21–26.
Purnamasari, D. (2018). The Emergence of Non-
communicable Disease in Indonesia. Acta Medica
Indonesiana, 50(4), 273–274.
Rahajeng, E., & Tuminah, S. (2009). Penelitian Prevalensi
Hipertensi dan Determinannya di Indonesia
. 580–587.
Vokonas, P. S., Kannel, W. B., & Cupples, L. A. (1988).
Epidemiology and risk of hypertension in the elderly:
the Framingham Study. Journal of Hypertension.
Supplement : Official Journal of the International
Society of Hypertension, 6(1), S3—9. http://euro
pepmc.org/abstract/MED/3216240
World Health Organisation (WHO). (2013). A Global Brief
on Hypertension: Silent Killer, Global Public Health
Crisis. https://doi.org/10.5005/ijopmr-24-1-2
ICSDH 2022 - The International Conference on Social Determinants of Health
160
