
A Comparative Study on the Observation Effect of Different
Performance CBCT on Mandibular Neural Canal
Xiaoyan Jiang, Pengbo Li and Bing Li
*
Yantai Stomatological Hospital, Yantai 264000, China
Keywords:
CBCT, Mandibular Neural Canal, Dental Implantst.
Abstract: CBCT products with different performance characteristics have great differences in imaging field of view and
detail performance capabilities. In this study, the CBCT imaging results of different performance parameters
are compared. The observation effect, position and direction of the mandibular neural canal were analyzed. It
provides a reference for the use of CBCT images in mandibular dental implant surgery. The selected
mainstream CBCT equipment can clearly image the mandibular neural canal, but the CBCT equipment with
a field of view of 8 cm or less cannot completely observe the entire mandibular neural canal.
1 INTRODUCTION
The position and orientation of the mandibular neural
canal is the focus of dental implantation in the
mandible. Traditional oral panoramic radiographs
(curved tomography) can show the position of the
mandibular neural canal and its relative relationship
with the surrounding teeth, but the overlapping and
deformation of anatomical structures in the images
often pose risks to the judgment of clinicians (Wang,
2019). Because of its advantages in imaging
principle, CBCT can obtain more accurate and clear
images of the mandibular canal.
The purpose of this study is to compare the
imaging performance of different equipments for
mandibular canal. It is expected to provide a reference
for the application of CBCT images in mandibular
implant surgery.
2 MATERIALS AND METHODS
2.1 Patient Information
CBCT imaging data of patients treated in Yantai
Stomatological Hospital from June 2021 to January
2022. The data screening criteria are as follows: The
patient has no history of mandibular fractures or
major surgery; The patient is over 18 years old; The
mandible has no metal objects that seriously affect
CBCT imaging and measurement, such as metal
correction brackets, amalgam fillings, etc.
After screening, 60 cases of CBCT data meeting
the research criteria were included, including 30
males and 30 females.
2.2 Equipment
The data used in this study were obtained using the
following equipment:
Equipment 1: Meyer, SS-X12008DPro-3D.
Scanning parameters: 115kV, 8mA, reconstruction
voxel size 0.25mm. Field of view size 23x18 cm.
Equipment 2: NewTom, VGi. Scanning
parameters: 110kV, 3mA, reconstruction voxel size
0.30mm. Field of view size 15x12 cm.
Equipment 3: Sirona, ORTHOPHOS XG 3D
CEPH. Scanning parameters: 90kV, 8mA,
reconstruction voxel size 0.16mm. Field of view size
8x8 cm.
Equipment 4: MORITA, Veraviewwpocs X550.
Scanning parameters: 90kV, 5mA, reconstruction
voxel size 0.16mm. Field of view size 8.8x8 cm.
2.3 Method
The observation effect of the mandibular neural canal
is analyzed from two aspects: First, whether the
mandibular neural canal can be clearly observed and
the position can be accurately judged; The second is
whether the mandibular neural canal can be
completely displayed in the field of vision.
Jiang, X., Li, P. and Li, B.
A Comparative Study on the Observation Effect of Different Performance CBCT on Mandibular Neural Canal.
DOI: 10.5220/0012012700003633
In Proceedings of the 4th International Conference on Biotechnology and Biomedicine (ICBB 2022), pages 41-45
ISBN: 978-989-758-637-8
Copyright
c
2023 by SCITEPRESS – Science and Technology Publications, Lda. Under CC license (CC BY-NC-ND 4.0)
41

In terms of clarity and location of the mandibular
canal, Clinically, the direction of the mandibular
neural canal varies. If the shape and position of the
mandibular neural canal can be clearly observed in
the CBCT image, we classify and record it according
to the following principles: Divide into 3 equal parts
from the top of the alveolar ridge to the upper edge of
the mandibular cortex. The one near the root of the
tooth is called the high position, the one close to the
cortical bone is called the low position, the one in the
middle is called the median position (Wang, 2019).
Patients were classified as "unobservable" if their
mandibular canal had low bone wall density or many
branches, making it difficult to determine its shape.
In the classification process, in addition to observing
the clarity and position of the mandibular neural
canal, anatomical parameters important for implant
surgery, such as the distance from the mandibular
neural canal to the alveolar process (canal ridge
distance), are also measured.
In terms of the integrity of the mandibular canal
observation, we marked the mental foramen on the
side of the jawbone clip as the anterior opening of the
mandibular canal, as shown in Figure 1; the
mandibular foramen on the lingual side of the jaw was
marked as the posterior opening of the mandibular
canal, as shown in picture 2. If the entire structure
between the anterior opening and the posterior
opening of the mandibular neural canal can be clearly
observed in the CBCT image, it is considered that the
entire neural canal can be observed completely;
otherwise, it is considered that the entire neural canal
cannot be completely observed.
Axial
Sagittal
Coronal 3D view
Figure 1: Anterior opening of the mandibular canal (mental foramen).
ICBB 2022 - International Conference on Biotechnology and Biomedicine
42
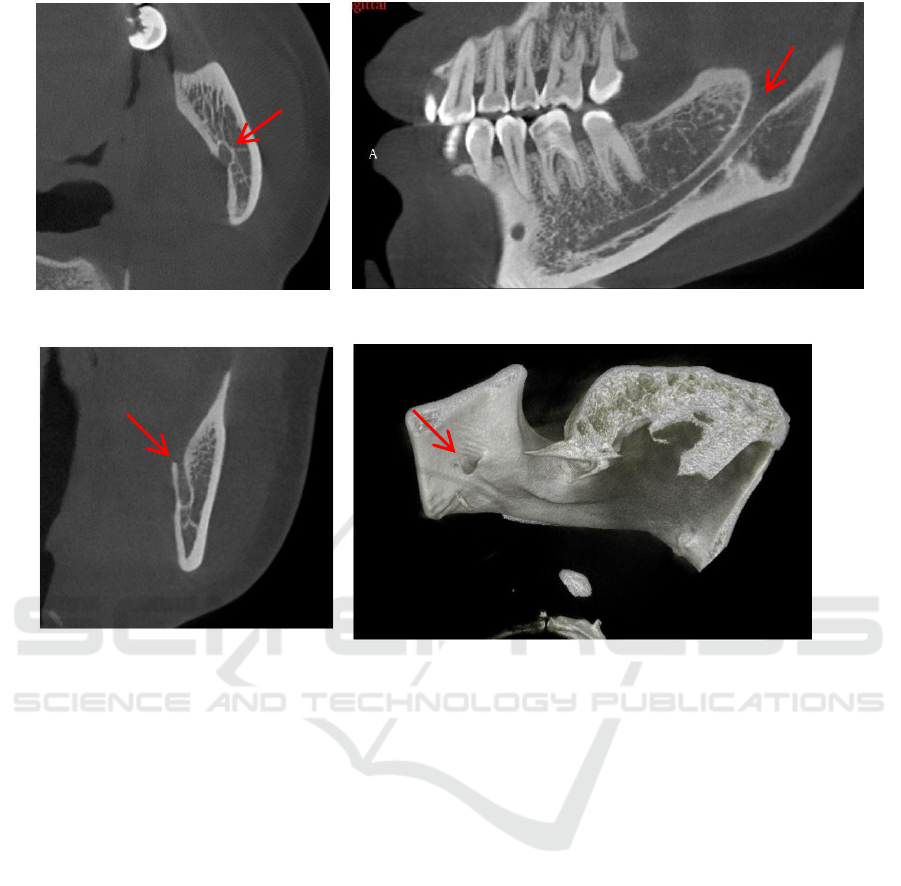
Figure 2: The posterior opening of the mandibular canal (mandibular foramen).
All imaging data were measured and analyzed by
2 imaging professionals, and the distance-related
quantitative values were measured 3 times and
averaged.
Statistical processing SPSS 20.0 statistical
software package was used to analyze the data, and
the selected specimens were strictly judged to control
selection bias. The Kappa test was used to test the
consistency of the measurement analysis results of the
two physicians: Kappa value greater than 0.8 and less
than or equal to 1.0, almost completely consistent;
Kappa value greater than 0.6 and less than or equal to
0.8, highly consistent; Kappa value greater than 0.4
and less than or equal to 0.6, moderately consistent ;
Kappa value greater than 0.2 and less than or equal to
0.4, general consistency; Kappa value greater than 0
and less than or equal to 0.2, extremely low
consistency. Wilcoxon paired signed rank was used
for difference analysis, and P<0.05 was considered
statistically significant.
3 TEST RESULTS AND
DISCUSSIONS
3.1 Whether the Mandibular Neural
Canal Can Be Clearly Observed
and the Position Can Be Accurately
Determined
The four CBCT devices selected in this study can
clearly observe the shape and position of the
mandibular neural canal in patients, and classify them
according to the position of the mandibular neural
canal. The evaluation of the clarity and position of the
mandibular neural canal by the two physicians was
"almost identical", and there was no significant
difference in the evaluation (P>0.05). Among the
selected samples, 24.5% had the mandibular canal in
the high position, 44.5% had the mandibular canal in
the middle, and 30.75% had the mandibular canal in
the low position.
Axial
Sagittal
Coronal 3D view
A Comparative Study on the Observation Effect of Different Performance CBCT on Mandibular Neural Canal
43

Table 1: Mandibular neural canal definition and location distribution.
able to observe clearly
high middle low
unable to
observe clearly
Equipment 1 25% 43% 32% 0 %
Equipment 2 24% 44% 32% 0 %
Equipment 3 24% 46% 30% 0 %
Equipment 4 26% 45% 29% 0 %
average value 24.5% 44.5% 30.75% 0 %
3.2 Whether the Mandibular Neural
Canal Can Be Completely
Observed
The four CBCT devices selected in this study have
significant differences in the imaging field sizes.
Among them: Device 1 has the largest field of view,
which can cover almost the entire skull below the
brow bone; Device 2 has a field of view that covers
the complete mandible and includes the
temporomandibular joint; Although the field of view
of Device 3 and Device 4 can completely cover the
entire dentition, because the field of view is too small
to show the entire mandible in the field of view. The
four CBCT devices selected in this study have
significant differences in the imaging field sizes.
Among them: Device 1 has the largest field of view
and can cover almost the entire head below the brow
bone; Device 2 has a field of view that covers the
complete mandible and includes the
temporomandibular joint. The field of view of device
3 and device 4 can completely cover the entire
dentition, but due to the small field of view, the entire
mandible cannot be displayed in the field of view, nor
the entire mandibular neural canal.
Because each device can clearly observe the
mandibular neural canal, the imaging field of view is
a key factor in determining whether the entire neural
canal can be completely observed. The diametrical
field of view is particularly critical. Device 1 and
Device 2 have a large enough field of view diameter,
so that the mandibular neural canal can be completely
distributed within the field of view diameter, so that
the entire mandibular neural canal can be observed,
which is more conducive to the safety of mandibular
implant surgery. Due to the limited field of view,
device 3 and device 4 can also meet the needs of
mandibular implant surgery, but cannot fully display
the second half of the mandibular neural canal, and
their clinical application scope is limited to a certain
extent.
Table 2: Imaging integrity of the mandibular neural tube.
Imaging field of view
Diameter (cm) x Height (cm)
Mandibular canal
imaging complete
Equipment 1 23 x 18
√
E
q
ui
p
ment 2 15 x 12
√
Equipment 3 8 x 8 x
Equipment 4 8.8 x 8 x
3.3 Discussion
The early observation and study of the three-
dimensional topography of the mandibular neural
canal mainly used spiral CT, especially the high-
resolution scanning mode (HRCT) in spiral CT. The
main observation items include the precise position of
the buccolingual, the height of the alveolar ridge, and
the contour of the bone plate. This information can be
summarized as the location, orientation, and
surrounding tissue of the mandibular neural canal
(Bai, 2008; Liu, 2014; Ge, 2003). In the impact data
of spiral CT, MPR images are mostly used for
observation, especially the sagittal images of the
posterior teeth. Although these methods can better
complete the preoperative observation of the
mandibular neural canal, the general equipment is
relatively expensive, and the spiral CT needs to be
shared with other departments, which limits the
clinical application.
With the popularization of oral CBCT equipment,
especially the convenience and high precision of oral
CBCT scanning, more and more physicians use
CBCT to observe and study the mandibular neural
ICBB 2022 - International Conference on Biotechnology and Biomedicine
44

canal. And it can completely cover the anatomical
information of the original spiral CT. The clear
observation of the mandibular neural canal in CBCT
can be applied in many clinical directions, such as
mandibular implant surgery, mandibular deformity
correction, impacted tooth extraction, mandibular
fracture treatment, etc. (Ye, 2013; Li, 2017; Li, 2019).
This study compared the application effects of
various CBCTs of different specifications in the
clinical observation of the mandibular neural canal.
Studies have shown that the four selected CBCT
devices with conventional performance can clearly
and accurately observe the shape and position of the
mandibular neural canal, which can meet the needs of
various clinical applications such as mandibular
implant surgery. But the field of view of these CBCT
products varies greatly, ranging from 23x18(cm) to
8x8(cm). The huge difference in the size of the field
of view results in a fundamental difference in the
integrity of the mandibular neural canal imaging, and
the small field of view will lead to the inability to
completely observe the position and direction of the
entire neural canal. According to clinical experience,
the length of the mandibular neural canal in adult
patients is generally 7 to 9 cm. In addition, the
incisors are generally required to be completely
displayed in the field of view during CBCT scanning.
At the same time, a small error in the positioning of
each patient is considered. Therefore, the diameter of
the task CBCT field of view should not be Less than
12 cm, in order to calmly observe the complete
direction of the mandibular neural canal. This study
suggests that CBCT can be well applied to the
observation of the mandibular neural canal, but to
observe the complete position and orientation of the
mandibular neural canal, a CBCT device with
sufficient field size should be used.
4 CONCLUSION
This study shows that the selected mainstream CBCT
equipments can obtain the clear image of the
mandibular canal. But, when the field of view is 8 cm
or below, the mandibular canal cannot be observed
intactly. Therefore, if the intact mandibular canal
needs to be observed, the CBCT device with a field
of view which is large enough should be choosed. The
diameter of the field of view should be given special
attention.
REFERENCES
Bai Gang, Chen Jiangang, Li Bo, Mandibular neural canal
CT scan and mandibular posterior teeth implantation
[J], Journal of Clinical Stomatology, August 2008, Vol.
24, No. 8, 481-483
Ge Gaohua, Mandibular nerve canal scanning method [J],
Youjiang Medicine, 2003, Vol. 31, No. 5, 433-434
Liu Handong, Application of multiple spiral CT in the
diagnosis of mandibular neural canal fractures in 56
cases, July 2014, 96
Li Tingting, Liu Yalin, Li Changyi, Overview of research
on bifurcated mandibular neural canal [J], Chinese
Journal of Geriatric Tone Medicine, November 2017,
Vol. 15, No. 6, 365-367
Li Lifeng, Shi Jingyi, Tu Junbo, etc., The positional
characteristics of the mandibular neural canal in the
mandibular angle and the significance of the machine
in the minimally invasive treatment of mandibular
angle fractures, Journal of Shanxi Medical University,
July 2019, Vol. 50, No. 7 period, 1025-1028
Wang Hu, Zheng Guangning, Oral Clinic CBCT Imaging
Diagnosis, People's Health Publishing House [M],
September 2019 First Edition: 246-247.
Ye Lijuan, Guo Fei, Kang Feiwu, etc., Cone beam CT
analysis of mandibular neural canal in patients with
mandibular protrusion[J], Journal of Oral and
Maxillofacial Surgery, August 2013, Vol. 23, No. 4,
271 -275
A Comparative Study on the Observation Effect of Different Performance CBCT on Mandibular Neural Canal
45
