
Acute Effects of Hypoxia and High Intensity Interval Exercise on
Health Promotion Among Male University Students
Xiaoyu Wei
1,2
, Xiaocong Liang
2,*
and Shiyi Wang
2
1
Faculty of Humanities and Social Sciences, Macao Polytechnic University, China
2
Beijing Institute of Technology, Zhuhai, Guangdong, China
Keywords: High Intensity Interval Exercise (HIIE), Hypoxia, Health Promotion.
Abstract: The aim of this study was to verify the acute effects of hypoxic high intensity interval exercise (HIIE) on
health promotion (Blood Pressure). Ten healthy university students participated and undertook the four
random exercise trials: rest in hypoxia (RH), rest in normoxia (RN), normoxic HIIE (NH), and hypoxic HIIE
(HH). Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were evaluated before and 30 min
after each trial. Both HH and NH led to post-exercise hypotension (PEH) during the post-test 30 minutes in
trials compared with RN trial, but the decrease magnitude of SBP and DBP did not reach significant trial
differences (p > .05). Significant decrease in SBP was only found in HH trial, and the duration of PEH in HH
was longer than that in NH during the 30-minute post-test observation. Exercise could make students feel
happier. HIIE can lead to PEH in both normoxic and hypoxic environment, while hypoxia strengthens this
effect. And HIIE help improve the affective feeling for university students.
1 INTRODUCTION
Almost 1.13 billion people in the world have
hypertension, of whom two-thirds are living in low-
and middle-income countries and hypertension is
claimed as a global public health crisis (World Health
Organization, 2021).
Studies have found that essential hypertension in
adults may originate in childhood. Prevention and
control of hypertension in adolescents can control the
occurrence and development of cardiovascular
disease in adults. University students are a very large
group of adolescents. If good living habits and
exercise methods are developed during their college
years, it not only will be beneficial for their physical
and mental health, but also has great significance to
the development of country education.
As such, researchers suggest that it is preventable
that blood pressure (BP) can be influenced by several
issues such as height, weight, fat, daily diet,
environment and physical activity (Diaz, 2013). The
benefit of low to moderate intensity endurance and
resistance exercise programs has been well supported
by previous researches (Cardoso Jr, 2010). However,
*
Corresponding author
Levinger and colleagues (Levinger, 2015) reported
that 60% of people could not meet the minimum-
recommended level of regular physical activity, in
which people found it difficult to spend at least 150
minutes per week in doing moderate-intensity aerobic
exercise. Hence, “no time” could be one of the main
barriers for adhering in regular low to moderate
intensity exercise programs.
Given this, high intensity interval exercise (HIIE),
are attracting more attention and interest from
university students. Hypoxic environment has been
suggested to be beneficial in clinical conditions such
as coronary artery disease and chronic obstructive
pulmonary disease (Burtscher, 2010). HIIE may
cause stronger decrease in BP in a hypoxic
environment after exercise. However, less studies
have paid attention to the BP responses after hypoxic
HIIE or normoxic HIIE.
Consequently, the purpose of
the current research was to compare the BP responses
and
affective feeling after hypoxic HIIE or normoxic
HIIE compared to the conditions of rest in hypoxia or
in normoxia in healthy male university students.
228
Wei, X., Liang, X. and Wang, S.
Acute Effects of Hypoxia and High Intensity Interval Exercise on Health Promotion Among Male University Students.
DOI: 10.5220/0012018800003633
In Proceedings of the 4th International Conference on Biotechnology and Biomedicine (ICBB 2022), pages 228-234
ISBN: 978-989-758-637-8
Copyright
c
2023 by SCITEPRESS – Science and Technology Publications, Lda. Under CC license (CC BY-NC-ND 4.0)

2 METHODOLOGY
The current research focused on the acute effects of
HIIE under hypoxic and normoxic environment on
the BP responses during and after a HIIE trial among
male university students. Additionally, this study
examined the correlations between BP responses and
individuals’ characteristics.
15 young physically inactive male university
students with normotensive BP were invited to
participate in the study. Finally, ten qualified male
participants were recruited and completed this study.
Subjects completed a brief medical history
questionnaire and a physical activity readiness
questionnaire prior to participation to rule out any
contraindications to performing vigorous exercise.
Details of exercise testing and risks associated with
the experimental procedures were explained to
subjects before they provide written inform consent.
2.1 Study Design
Prior to the experiment, participants were invited to
present to the laboratory for an initial visit in order to
be familiar with the procedures of the experiment and
to complete the anthropometric measurements.
During this session, height (cm), weight (kg), body
composition, and resting BP were measured. Subjects
also completed a bout of cycling sprint on a cycle
ergometer (Wingate Anaerobic Test protocol).
During the next four visits, participants were asked to
complete randomly the main experimental
conditions—rest in hypoxia (RH), rest in normoxia
(RN), normoxic HIIE (NH), and hypoxic HIIE (HH).
All trials were separated by at least two days and
conducted during 5PM and 9PM. All the four trials
were performed in one month to ensure the similar
physiological conditions.
Participants were asked to maintain free-living
conditions during the experimental period and be
instructed to abstain from strenuous exercise and
consumption of alcohol for 24 hours, caffeine for 12
hours, and food for 2 hours before the beginning of
each trial. Daily activities were recorded in a diary of
the prior 48 hours before each trial. The levels of
light, humidity, and atmospheric pressure in the
laboratory were controlled to remain stable, and the
temperature was controlled at 20℃.
During the periods when a trial started five
minutes before and 30 minutes after, participants
were asked to be seated on a chair and listened to the
rhythm of 24 BPM and in an upright seated position
for the recording of ambulatory BP measurement.
HIIE consisted of two 30-second bouts of sprint
exercise on a cycle ergometer (Monark Ergomedic
894E, Monark, Sweden) separated by four minutes of
recovery. Participants performed the sprints against a
braking force calculated as the kilogram of body mass
multiplied by 0.075. The simulated hypoxia
(AltiTrainer, SMTEC, Switzerland) was set to be
equal to 2500m altitude. Subjects wore breathing
masks one minute before the test. Additionally, mask
was taken off immediately when the exercise ended.
HR, Ratings of Perceived Exertion (RPE), Affective
Scale and Blood Oxygen Saturation (SO2) were
recorded during the experiment.
Participants remained seated for 10-minute period
of rest before moving to the ergometer and being
matched with Portapres device (Portapres Model 2,
TNO Biomedical Instrumentation, Amsterdam,
Netherlands). After the exercise, participants seated
on the chair for 30 minutes for recording. Subjects
were asked to rest on the chair immediately after the
exercise.
2.2 Statistical Analysis
Statistical analyses were performed using SPSS 20.0
for Windows (SPSS Inc., Chicago, Chicago, Ill.,
USA). Data was reported as mean ± SD. Statistical
significance was assumed at p < 0.05.
3 RESULTS
3.1 Subject Characteristics
Initially, 15 individuals were invited to participate in
the study. Five of these potential participants were
removed from the experiments as they did not meet
the inclusion criteria for medical history (n=1), daily
physical activity (n=2), or dropped out for personal
reasons (n=2), leaving ten participants for final
participation. All the enlisted participants (n=10)
completed the study, and anthropometric and
descriptive results are presented in Table 1. Exercise
data is shown in Table 2.
Table 1: Subjects Characteristics.
Mean Std. Deviation
Age (year) 23.70 1.06
Height (cm) 173.5 5.26
Weight (kg) 67.37 5.91
BMI (kg/m
2
) 22.36 1.09
Fat (%) 16.03 2.66
VO
2peak
(ml/kg/min) 37.20 5.37
Acute Effects of Hypoxia and High Intensity Interval Exercise on Health Promotion Among Male University Students
229

Table 2: Power Output and Rate of Fatigue for Sprinting Exercise.
NH HH
1_Sprint 2_Sprint 1_Sprint 2_Sprint
Absolute PP (W) 667±149 625±113 611±74.1 588±86.9
Relative PP (W/Kg)
9.99±2.44 9.31±1.68 9.14±1.49 8.75±1.30
Absolute MP (W) 454±86.1
*
403±69.8 424±45.3 399±51.1
Relative MP (W/kg) 6.76±1.29
*
5.99±0.96 6.31±0.55 5.91±0.45
Rate of fatigue (%) 84.1±17.7 83.8±16.3 89.2±17.8 76.4±17.1
Note.
*
p < .05 PP: peak power MP: mean power
3.2
BP Responses to Acute Hypoxia and
HIIE
Pre-test values of SBP and DBP of the four trials were
compared in order to ensure that these pre-test values
were approximately identical. Results showed that the
pre-test values of SBP and DBP were not
significantly different among all trials (p > 0.05).
These results, therefore, supported that the pre-
exercise BPs of all trials are not varied with each
other. The results are shown in Table 3.
Table 3: Pre-test Values of BP Values.
RN RH NH HH
p
SBP
(
mmH
g)
122±9 123±8 122±8 123±7 0.914
DBP
(
mmH
g)
68±5 65±5 65±5 66±5 0.966
3.3
SBP Responses After Test
The changes of post-test SBP values are shown in
Figure 1. Among four trials significant differences (p
< .01) were found during the 1 to 5, 26 to 27, and 29
to 30 minutes and significant differences were found
during the 16 to 17, 20, and 28 minutes.
During 1 to 5 minutes, SBP increased
significantly. Specifically, SBP in the NH trial
significantly increased compared with RN trial (ps <
.05, .01 or .001) during 1 to 4 minutes and RH trial
(ps < .05, .01 or .001) during 1 to 5 minutes. SBP in
the HH trial significantly increased compared with
RN trial (ps < .05 or .01) during 1 to 3 minutes and
RH trial (ps < .01 or .001) during 1 to 4 minutes. SBP
significant decreased after post-test 16 minutes. In
post-test 17, 26, 27, and 30 minutes, significant
differences were found between HH and RN (p <
.05); in post-test 16, 28, and 29 minutes, marginal
significant differences were found between HH and
RH (p = .077, .084 and .055, respectively). However,
no significant differences were found among NH, RN
and RH (p > .05) tests during the post-test 30 minutes,
and the same as NH and HH tests.
Note. SBP value of RN was not included in the figure as it was set to be the baseline level (i.e. zero) for the analyses.
a All values during the 30-minute recovery were separated into one data point using an interval of every minute.
* p < .05. ** p < .01. *** p < .001
Figure 1: Changes of Post-test SBP Values Compared with RN.
ICBB 2022 - International Conference on Biotechnology and Biomedicine
230
3.4
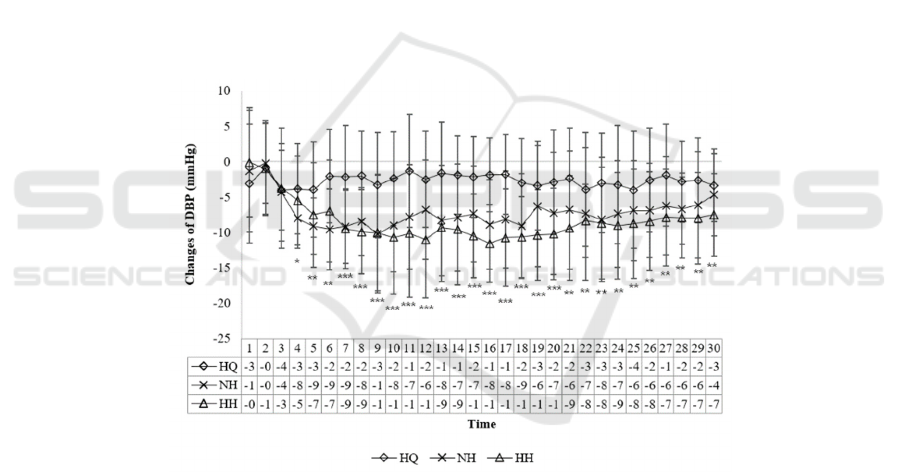
DBP Responses After Test
The changes of post-test DBP values are shown in
Figure 2. During the 30-minute observation after the
tests of the four trials, significant results were found
for most of the time period except during post-test 1
to 3 minutes (p > .05). After the 4th minute,
significant or highly significant differences were
found among the four trials (ps < .05, .01 or .001).
During the 30 minutes recovery, DBP values were
significantly decreased in the NH trial compared with
RN trial (p < .01) in the post-test 4 to 8 minutes; DBP
in NH significantly decreased compared with RN (p
< .05) in the post-test 9, 10, 13, 15 to 18, and 28
minutes; DBP in NH had decreased at a marginal
significant level compared with RN trial in the post-
test 14 (p = .055) and 26 (p = .054) minutes. DBP in
NH trial were highly significantly decreased
compared with RH (p < .01) in the post-test 10 and 16
minutes; DBP in
NH were significantly decreased
compared with RH (p < .05) in the post-test 8, 11, 13,
and 14 minutes; the changes of DBP in NH were
marginal significantly decreased compared with RH
in the post-test 12 (p = .065), 15 (p = .067), and 17 (p
= .054) minutes.
DBP in HH trial significantly decreased compared
with RN (p < .01) in the post-test 7, 8, and 15 to 22
minutes; DBP in HH trial significantly decreased
compared with RN (p < .05) in the post-test 9, 10, 12
to 14, and 23 to 30 minutes; DBP in HH trial had
decreased at a marginal significant level compared
with RN in the post-test 5 (p = .061) and 6 (p = .076)
and 11 (p = .057) minutes. DBP in HH trial
significantly decreased compared with RH (p < .01)
in the post-test 15, 16 and 19 minutes; DBP in HH
significantly decreased compared with RH (p < .05)
in the post-test 11 to 14, 17, and 18 minutes; DBP in
HH had decreased at a marginal significant level
compared with RH in the post-test 20 (p = .054)
minute. However, no significant differences were
found between RN and RH (p > .05) tests during the
post-test 30 minutes, and the same as NH and HH
tests.
Note. DBP value of RN was not included in the figure as it was set to be the baseline level (i.e. zero) for the analyses.
a All values during the 30-minute recovery were separated into one data point using an interval of every minute.
* p < .05. ** p < .01. *** p < .001.
Figure 2: Changes of Post-test DBP Values Compared with RN.
3.5
The Analysis of AUC
The previous results (Figure 1) showed that SBP was
significantly higher than normal situation during the
one to five minutes among the four trials, hence
indicating that BP values did not recover from the
tests. As such, the AUC was calculated from the 6th
minute (Table 4). After analysis, the AUC in SBP did
not have significant differences among the four tests
(p > .05). However, for DBP, significant differences
was found among the four tests (p < .001).
Sidak post hoc tests revealed that the AUC of
DBP in HH trial significantly decreased compared
with RN (p = .004), RH (p =.018) and NH (p = .023)
trials. AUC of DBP in NH trial significantly
decreased compared with RN trial (p = .022) and had
decreased at a marginal significant level compared
with RH (p = .077) trial.
Acute Effects of Hypoxia and High Intensity Interval Exercise on Health Promotion Among Male University Students
231

Table 4: The AUC after Test.
AUC RH NH HH
SBP
(mmHg*min)
-5±195 -58±131 -121±204
DBP
(mmHg*min)
***
-63±140 -187±153 -230±142
Note. BP values of RN were not included in the table as it
was set to be the baseline level (i.e. zero) for the analyses.
***
p < .001
3.6 Analysis of Impact Factors of PEH
Multiple stepwise regression analysis was performed
to examine the relationships between independent
variables, including body composition (i.e. weight,
height, BMI, and fat), VO2peak, mean power in the
two sprint exercise, and dependent variables,
including the AUC of SBP, DBP, and MAP, after
normoxic and hypoxic HIIE.
One significant result was found among all
multiple regression analyses (Table 5). Regression
analysis showed that the AUC of SBP in hypoxic
HIIE can be significantly influenced by independent
variables including body composition (i.e. weight,
height, BMI, and fat), VO2peak, and mean power in
the two sprint exercise. All the independent variables
accounted for 92.3% the total variance of AUC of
SBP in hypoxic HIIE. Among the total variance, body
composition including weight, height, BMI, and fat,
explained 77.7% among 92.3% of the variance.
However, adding VO2peak and mean power into the
model only explained 4% and 6.6% more of the total
variance, respectively. Hence, VO2peak and mean
power did not have much influence on the AUC of
SBP in HH trial. Body composition is the most
important independent.
Table 5: Regression of AUC of SBP in HH.
Unstandardized Coefficients
Standardized
Coefficients
t Sig.
B Std. Error
β
Model 1: R
2
= 0.777, F = 8.852, p = 0.017
*
Constant 155043.692 31839.918 4.869 0.005
weight 1139.627 234.202 33.037 4.866 0.005
height -865.446 179.22 -22.334 -4.829 0.005
BMI -3701.543 739.998 -19.751 -5.002 0.004
Fat 58.419 21.35 0.763 2.736 0.041
Model 2: R
2
= 0.812, F = 8.776, p = 0.028
*
Constant 137728.481 31802.048 4.331 0.012
weight 1014.177 233.385 29.4 4.346 0.012
height -769.375 178.615 -19.855 -4.307 0.013
BMI -3334.626 729.452 -17.793 -4.571 0.01
Fat 85.718 27.783 1.119 3.085 0.037
VO
2peak
12.405 8.942 0.327 1.387 0.238
Model 3: R
2
= 0.923, F = 16.371, p = 0.059
c
Constant 147999.297 31410.378 4.712 0.042
weight 1076.648 234.76 31.211 4.586 0.044
height -833.144 176.183 -21.5 -4.729 0.042
BMI -3505.597 712.354 -18.705 -4.921 0.039
Fat 76.804 22.607 1.003 3.397 0.077
VO
2peak
18.45 8.106 0.486 2.276 0.151
MeanPower_1
a
-1.625 0.87 -0.362 -1.869 0.203
MeanPower_2
b
2.536 1.034 0.636 2.453 0.134
Note. The dependent variable is AUC of SBP in HH trial. The independent variables in model 1 are the body composition, including
weight (kg), height (cm), BMI (kg/m
2
), and fat (%). The independent variables in model 2 are the body composition and VO
2peak
(ml/kg/min) which represents cardiopulmonary function. The independent variables in model 3 are the body composition, VO
2peak
,
and the mean power (Watt) in the two sprint exercise.
a
the mean power in the first sprint.
b
the mean power in the second sprint.
c
marginal significant difference.
*
p < .05.
ICBB 2022 - International Conference on Biotechnology and Biomedicine
232

3.7 Post-Exercise Affective Evaluation
Subjective feeling was evaluated after hypoxia and
normoxic HIIE using Affective Scale. The feeling of
happiness were significantly increased after NH and
HH compared with RN.
Table 6: Affective evaluation results.
RN RH NH HH
Affectiv
e scale
0±0.8
2
0.33±0.8
2
3.89±0.99
*
**
4±0.47
*
**
Note.
***
p < .001
4 DISCUSSION
The current study proved that acute hypoxic HIIE in
hypoxic condition resulted in a more effective
decrease in BP compared with normoxic condition.
This is the first study to compare the acute effects of
hypoxia and HIIE on PEH in male university
students.
In the current study, DBP was found to have a
significant decrease in normoxic HIIE compared with
rest in normoxia trial, but the decrease in SBP did not
reach the significant level. As the higher exercise
intensity and longer duration can result in greater
PEH (Cote, 2015; Eicher, 2010), this could the reason
that only DBP was found decreased in this research.
More importantly, the present study found that
HIIE led to PEH in both normoxic and hypoxic
environment, while hypoxia strengthened this effect.
In this study, the magnitude of PEH did not reach
significant differences between NH and HH, but the
duration of PEH was not at identical level in the two
tests. Significant decreases in SBP were found in
totally four minutes separated amongst the 30-minute
observation after HH trial, compared with the RN
trial. Kaplan (Kaplan, 2000) contended that SBP
value alone has been recognized as an important
cardiovascular risk factor. Other scholars also agreed
that high SBP is more dangerous than high DBP alone
in determining the risk of cardiovascular disease
(Pescatello, 2004). Therefore, the current results that
SBP was significantly decreased after hypoxic HIIE
showed that effect of hypoxia might be an important
factor in decreasing SBP.
In the changes of the post-exercise DBP,
significant levels of PEH were found in totally 23
minutes and 13 minutes separated amongst the 30-
minute observation after HH and NH trial,
respectively, compared with the baseline level of RN
trial. Moreover, significant levels of PEH were found
in totally 11 minutes and six minutes separated
amongst the 30-minute observation after HH and NH
trial, respectively, compared with the baseline level
of RH trial. In the current study, HIIE in both
normoxic and hypoxic environment caused
significant decreases in DBP. This study also found
that HH trial had a longer duration of PEH than NH.
Meanwhile, these results showed the durations of
PEH in DBP in HH trial were longer than NH trial
during all 30 minutes of post-exercise observation.
These results may support the argument that HIIE in
hypoxia has a greater effect on PEH than normoxia.
On the other hand, the current research also
examined the AUC, which was claimed as another
novel and robust approach to quantify PEH. Liu (Liu,
2012) proved that the AUC of BP was significantly
associated with peak BP decrease. In the current
study, AUC of DBP was found significantly higher in
HH trial than in NH trial, which implied that HIIE in
hypoxia caused a greater extent of PEH compared
with HIIE in normoxia.
Finally, the results of multiple stepwise regression
analyses showed that only AUC of SBP in HH trial
was significantly influenced by the model composed
of body composition (i.e. weight, height, BMI, and
fat), VO2peak, and mean power in the two sprint
exercise. This result partially supported the fifth
hypothesis. On one hand, BMI had a negative
relationship with AUC of SBP in HH trial, which
implied that decreasing BMI would lead to greater
AUC after hypoxic HIIE protocol. On the other hand,
weight and fat both had positive relationship with
SBP after hypoxic HIIE. In Forjaz and colleagues’
study (Forjaz, 2000), it was found that the magnitude
of PEH was stronger for participants with lighter
weight and lower BMI. Nonetheless, in this study,
greater PEH was discovered in participants of more
weight and fat. This might be attributed to the fact that
weight and BMI could not represent all dimensions of
the body composition, because the relationship
between BMI and body fat could be influenced by
age, gender, ethnicity and race (McArdle, 2010).
Nonetheless, the percent of body fat was not
measured in their research, therefore, BMI might not
accurately reflect the proportion of fat in the body
composition, which might explain the unexpected
relationship among weight, BMI, and fat and AUC of
SBP after hypoxic HIIE.
Moreover, VO2peak and the mean power did not
have the significant relationship with the dependent
variables, implying that the AUC of SBP after
exercise was largely accounted by body composition,
instead of cardiopulmonary function and exercise
Acute Effects of Hypoxia and High Intensity Interval Exercise on Health Promotion Among Male University Students
233

performance. Also, this relationship was only found
significant in HH trial, which suggested that hypoxic
condition was an important factor that strengthened
the effect of HIIE. Meanwhile, limited studies have
explored the relationships among participants’ body
composition, VO2peak and PEH. Consequently,
more studies are needed to figure out these
relationships.
Mental health problems among university
students is an emerging public health issue (Winzer,
2018). This study also found that the HIIE could
significantly enhance the feeling of happiness for
university students, which can be used for students to
relieve academic pressure and has an important role
in improving students' mental health.
5 CONCLUSION AND
SUGGESTIONS
This research examined the acute effects of hypoxic
condition and HIIE on both physical and mental
health improving in inactive male university students.
While HIIE in normoxic environment could lead to
decrease in DBP, HIIE in hypoxic environment could
decrease SBP and DBP. Although the difference of
the decrease in SBP and DAP among NH and HH trial
did not reach significant level, significant decrease in
SBP was only found in HH trial. Moreover, the
duration of PEH in HH was longer than that in NH
during the 30-minute post-test observation.
Therefore, hypoxic HIIE seems to be a more effective
method to decrease BP than normoxic HIIE, which
might serve as a protective mechanism against
cardiovascular risk and the development of
cardiovascular disease. This effective exercise
method can be applied to university students to
improve their physical function and mental state.
Although hypoxia condition is hard for students for
training, but it could be applied to cardiovascular
disease patients, athletes or other special groups.
While this study only performed 30 minutes
observation of post-exercise data collection, previous
research found a small difference in the peak PEH
response after one hour and 30 minutes of HIIE
(Rossow, 2010). Future research may consider having
a longer observation of post-exercise BP response in
order to provide more evidence of PEH. In addition,
current research only involved ten participants. The
small sample size might be a reason that some
variables such as SBP did not have significant
difference. Accordingly, further studies may consider
recruiting more participants.
In addition, as PEH could be affected by exercise
intensity (Bonsu, 2016), hypoxic environment (Wee,
2015), and participants’ characteristics (Halliwill,
2001), future studies could perform different HIIE
protocols with various intensity and duration and
different levels of hypoxic exposure, in different
gender in order to examine the effect of exercise on
physical and mental health.
REFERENCES
A.T. Cote. S.S. Bredin. A.A. Phillips. M.S. Koehle. D.E.
Warburton. Eur. J. Appl. Phy. 115, 81-89. (2015)
B. Bonsu. E. Terblanche. Eur. J. Appl. Phys. 116, 77-84
(2016)
C.G. Cardoso Jr, R.S. Gomides, A.C.C. Queiroz, L.G.
Pinto, F.D.S. Lobo, T. Tinucci, ... & C. L. D. M. Forjaz,
Cli. 65, 317-325. (2010).
C.L.M. Forjaz. T. Tinucci. K.C. Ortega. D.F. Santaella. D.
Mion Jr. C.E. Negrão. Blo. Pres. Mon. 5, 255-262
(2000)
I. Levinger, C.S. Shaw, N.K. Stepto, S. Cassar, A.J.
McAinch, C. Cheetham, & A.J. Maiorana, Clin. Med.
Ins.: Card. 9, 53-63. (2015).
J.D. Eicher. C.M. Maresh. G.J. Tsongalis. P.D. Thompson.
L.S. Pescatello. Ame. Hea. J. 160, 513-520. (2010)
J. Wee, M. Climstein, J. Sci. Med. Spo. 18, 56-61 (2015)
J.R. Halliwill. Exe. and Spo. Sci. Rev. 29, 65-70 (2001)
K.M. Diaz, & Shimbo D. Cur. Hyp. Rep. 15, 659-668.
(2013).
L.S. Pescatello. M.A. Guidry. B.E. Blanchard, A. Kerr. A.L.
Taylor. A.N. Johnson. P.D. Thompson. J. Hyp. 22,
1881-1888. (2004)
L. Rossow. H. Yan. C.A. Fahs. S.M. Ranadive. S.
Agiovlasitis. K.R. Wilund. B. Fernhall. Amer. J. Hyp.
23, 358-367. (2010)
M. Burtscher. H. Gatterer. C. Szubski. E. Pierantozzi. M.
Faulhaber. Sle. Bre. 14, 209-220. (2010)
N.M. Kaplan. Cir. 102, 1079-1081. (2000)
R. Winzer. L. Lindberg. K. Guldbrandsson, A. Sidorchuk.
PeerJ, 6, e4598 (2018)
S. Liu. J. Goodman. R. Nolan. S. Lacombe. S.G. Thomas,
Med. Sci. Spo. Exer. 44, 1644-52. (2012)
World Health Organization. (2021). Improving
hypertension control in 3 million people. Retrieved
from
https://apps.who.int/iris/rest/bitstreams/1311822/retrie
ve
W.D. McArdle. F.I. Katch. V.L. Katch. Exercise
physiology: Nutrition, energy, and human
performance. (Wolters Kluwer-Lippincott Williams &
Wilkins Health, 2010)
ICBB 2022 - International Conference on Biotechnology and Biomedicine
234
