
Analysis of the Current Situation and Problems of China's National
Infectious Disease Network Direct Reporting System Under the
COVID-19
Chang Liu
1
, Yuanshan Liang
2
and Mengqi Zhu
3
1
Macao Polytechnic University, Faculty of Humanities and Social Science, Macao SAR, 999078, China
2
Guangdong University of Foreign Studies, Academy of International and Regional Studies, Guangzhou, 510000, China
3
Xuchang Central Hospital, Department of Geriatrics, Xuchang, 461000, China
Keywords: Infectious Disease Epidemiology, Surveillance systems, National Infectious Disease Reporting System.
Abstract: Considering the highly transmissible feature of infectious diseases, each country establishes its surveillance
system for infectious diseases to restrain the spread of infectious diseases quickly. This is the first step of
humanity’s “war against epidemics”. This paper briefly reviews the development of China's national
infectious disease network direct reporting model. From the early days of handwriting and mail delivery to
the world’s largest direct reporting system for infectious diseases, China’s digital government has brought a
huge breakthrough in preventing infectious diseases. However, the direct reporting system for infectious
diseases, which was claimed to be able to reach the National Centre for Disease Control and Prevention in
China within 2 hours, did not work as expected during the early outbreak of “COVID-19” in early 2020.
Therefore, this paper explores the basic reasons for the “non-functioning” of the network direct reporting
system and, hence, discusses the problems of digital government in infectious disease surveillance and the
important role of advanced technology in infectious disease surveillance systems. Finally, suggestions are
made for the direct reporting system of infectious disease networks in China.
1 INTRODUCTION
The Chinese Ministry of Health officially launched
Decree No. 37 on January 1, 2004, on the
implementation of the Measures for the
Administration of Information Reporting on
Surveillance of Public Health Emergencies and
Infectious Diseases, followed by the opening of a
direct network reporting system based on case
reporting of infectious diseases throughout the
country, which means that the information network is
extended to townships (towns) and urban
communities through national, provincial, municipal
and county disease prevention and control agencies,
thus forming a vertical and horizontal information
reporting network (Li & Zhang, 2011). The
innovative management model of reporting
epidemics directly from the most grassroots medical
and health institutions to the National Centre for
Disease Prevention and Control (NCDC) has become
a breakthrough in the information management
model in China's public health sector, improving the
early detection of abnormal information through real-
time monitoring of epidemics, especially plays an
important role in the prevention, control, and disposal
of infectious disease epidemics, the safeguarding of
major rally events and the prevention of epidemics
during natural disaster relief.
2 REVIEW OF THE EPIDEMIC
OUTBREAK REPORTING
METHODS IN CHINA
China’s statutory epidemic reporting and feedback
system was established in the 1950s when the
Chinese State Council approved a bill to establish
Health Protection Stations (HEPS) nationwide. Since
1952, the Ministry of Health issued a series of health
statistics forms, including the Basic Health
Information Form, the Infectious Disease Form, the
Hospital Work Form, the Hospital Inpatient Disease
Classification Form, and the Population Injury and
648
Liu, C., Liang, Y. and Zhu, M.
Analysis of the Current Situation and Problems of China’s National Infectious Disease Network Direct Reporting System Under the COVID-19.
DOI: 10.5220/0012041400003620
In Proceedings of the 4th International Conference on Economic Management and Model Engineering (ICEMME 2022), pages 648-653
ISBN: 978-989-758-636-1
Copyright
c
2023 by SCITEPRESS – Science and Technology Publications, Lda. Under CC license (CC BY-NC-ND 4.0)
Death Statistics Form. Subsequently, the Chinese
Academy of Medical Sciences (CAMS) was
established in 1956 and the Chinese Academy of
Preventive Medicine (CAPM) in 1986, both of which
are responsible for the collection, management,
analysis, and feedback of infectious disease
surveillance data throughout China(Wang, 1996).
Before 1985, infectious disease surveillance in China
was conducted in the most primitive way, that is,
clinicians filled out “infectious disease report cards”
manually, and then reported and summarized
statistics by mail through health prevention stations
in villages, towns, counties, cities, provincial, and
national levels (from county health bureau to city
health bureau, to provincial health bureau, and finally
to CAPM)(Xu & Chen, 2020). In other words, it often
takes more than a month, or even longer, for
information about the infectious disease to reach
decision-makers. In the 1970s, China set up a single
disease surveillance system for influenza, AIDS, and
malaria, followed by a comprehensive disease
surveillance system in the 1980s, with 145 disease
surveillance sites nationwide, monitoring four areas:
birth, death, and infectious disease incidence, and
planned immunization (Ma et al., 2006).
By the year 1986, there has been an initial
electronic reporting system of infectious diseases in
China, with more than 200 network nodes nationwide
implementing monthly electronic reporting of
national statutory infectious diseases, and some
provinces even began using e-mail as a more efficient
reporting method. In 2002, the Chinese Academy of
Preventive Medicine (CAPM) was officially
renamed the National Centre for Disease Control and
Prevention (NCDC). According to the Law of the
People’s Republic of China on the Prevention and
Control of Infectious Diseases (2004), CDCs at all
levels are responsible for the surveillance, prediction,
epidemiological investigation, and notification of
epidemics and other prevention and control work of
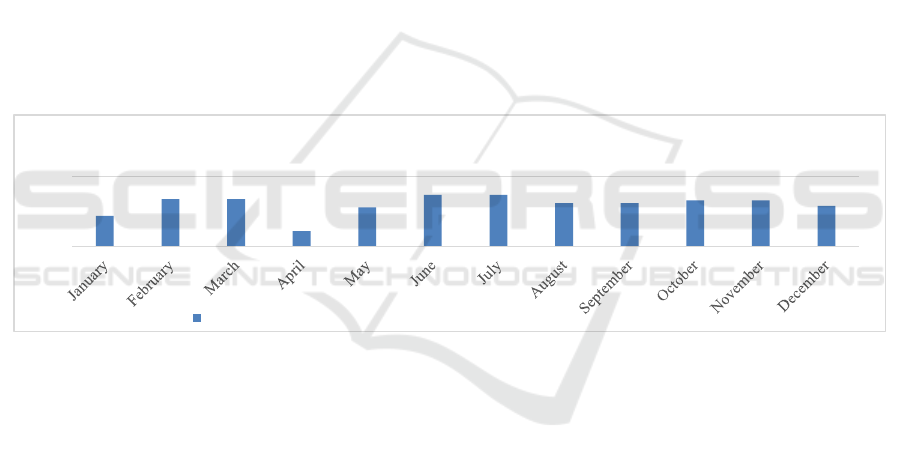
infectious diseases. Based on the official data from
the NCDC, the epidemic dynamic results of 35
statutory infectious diseases analyzed by the national
disease surveillance sites in 2000 is shown in figure
1.
Figure 1: The epidemic situation of 35 statutory infectious diseases in national disease surveillance sites in 2000.
It can be seen that the lowest reporting rate of 35
statutory infectious diseases at the national disease
surveillance sites from 2000 to 2002 was 77.08% in
April 2000, and the highest reporting rate was
95.14% in June and July 2000. There were no months
with a 100% reporting rate during this period. In
2003, after the SARS crisis, the NCDC established
the National Network Direct Reporting System
(NDRS) for infectious diseases and public health
emergencies with the database of infectious diseases
and public health emergencies as the core, according
to the construction principle of “horizontal to the
edge and vertical to the bottom” through the
reorganization and transformation of the epidemic
reporting procedure (Huang et al., 2008). “Vertical to
the end” means that all health institutions above the
township level are included in the system and entitled
to log in and fill in the information reported;
“horizontal to the edge” means that all health
institutions in the country are covered, including
medical, supervision, disease prevention, and control
institutions. According to the official data from the
NCDC, the system has been used by all health
institutions in China. According to the official data of
the NCDC, the dynamic analysis of the epidemic
situation of 37 statutory infectious diseases at the
national disease surveillance sites in 2006 is shown
in figure 2.
122
134 134
111
128
137 137
131 131
133 133
129
100
150
data analysis of 35 statutory infectious diseases in national disease surveillance sites in
2000
The actual number of copies of reports received (144 copies should be received)
Analysis of the Current Situation and Problems of China’s National Infectious Disease Network Direct Reporting System Under the
COVID-19
649
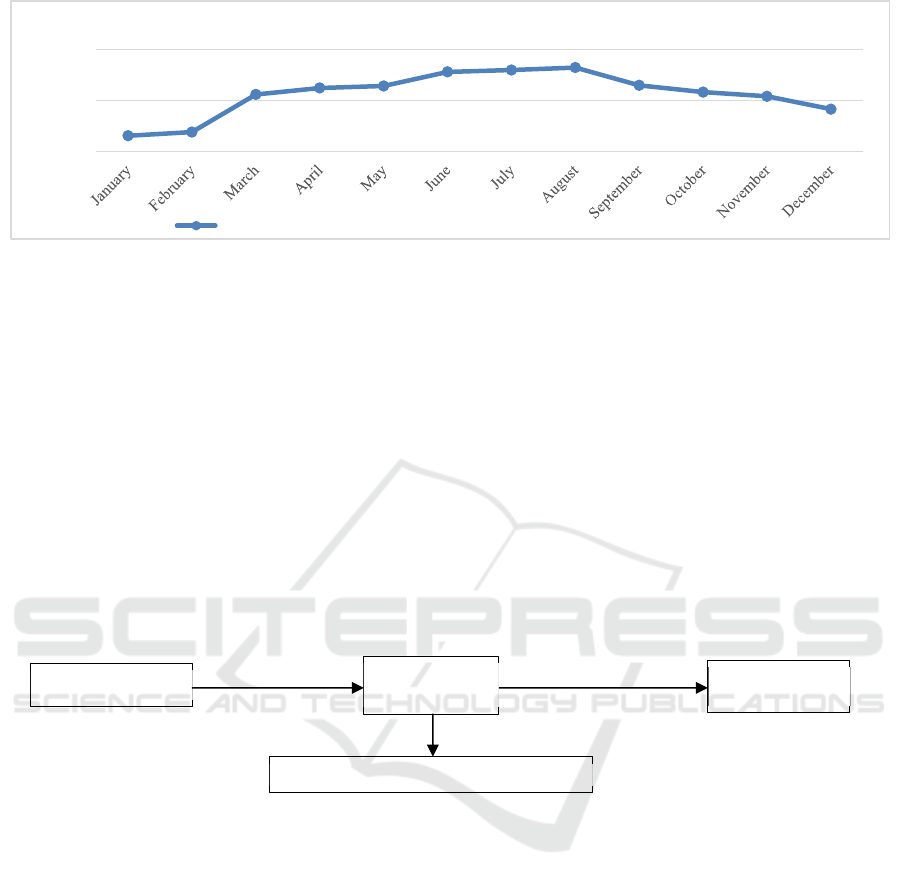
Figure 2: Epidemiological trends of 37 statutory infectious diseases in national disease surveillance sites in 2006.
Since the digital government model was initiated,
the number of report cards has increased abruptly,
with the lowest number of monthly report cards in
2006 being over 300,000 and the highest number of
report cards close to 600,000. The increase in the
number of infectious disease report cards means that
China’s ability to monitor infectious diseases has
improved, and reflects the positive effect that the
digital government has brought to infectious disease
surveillance. On September 29, 2017, the
“Development of China’s Public Health as an
Essential Element of Human Rights (2017)” stated
that China has built the world’s largest online direct
reporting system for notifiable epidemic diseases and
public health emergencies. The epidemic disease
reporting system covers 71,000 medical institutions,
with 160,000 users and nine million annual
individual reports. Development of health and
progress of human rights in China describes that the
country has set up a laboratory network comprised of
disease control and prevention institutions at the
national, provincial, city, and county levels.
Influenza, poliomyelitis, measles, and meningitis B
labs of the NCDC have become WHO reference labs.
According to the above tables, we can briefly
draw the network direct reporting process stipulated
in the “Administrative Measures for Monitoring
Information Reporting of Public Health Emergencies
and Infectious Disease Epidemic Situations”, as
shown in the following.
Figure 3: Direct network reporting process as stipulated in the Measures for the Management of Information Reporting on
Surveillance of Public Health Emergencies and Infectious Diseases (image source: the author’s self-made).
It is clear that before 2020, the major reporters for
China’s direct infectious disease network reporting
system were either the hospitals to which the primary
clinicians belonged or the local CDCs at the county
level or above. However, the COVID-19 outbreak in
early 2020 was not initially reported through the
direct infectious disease network reporting system,
and this issue will be addressed and analyzed in the
following sections.
3 CASE STUDY
At the end of 2019, Hubei Provincial Hospital of
Integrated Traditional Chinese and Western
Medicine found several family-like cases of
pneumonia of unknown cause. On December 27, the
hospital reported to the Wuhan Jianghan District
CDC. On December 29, the hospital conducted the
first joint expert consultation, and then the hospital
reported the situation to the provincial and municipal
health commission yet did not report it through the
network direct reporting system(2020). On
December 30, the Wuhan Municipal Health
Commission issued the internal departmental
guidance documents “Emergency Notice on
Reporting the Treatment of Unexplained
Pneumonia” and “Emergency Notice on Doing a
Good Job in the Treatment of Unexplained
Pneumonia”. A comprehensive and retrospective
investigation of seafood market-related pneumonia
cases was launched. On the same day, Li Wenliang,
311965
326035
473818
499198
507110
562515
569824
579696
509725
482945
466430
416211
250000
450000
650000
data analysis of 37 statutory infectious diseases in national disease surveillance sites in
2006
The actual number of copies of reports received (144 copies should be received)
If there is no network direct
reporting system account
If there is a network direct
reporting system accoun
t
Organizing expert
consultation
Primary Clinician
Departments/
Hospitals
Direct network
re
p
ortin
g
Local CDC does direct network reporting
ICEMME 2022 - The International Conference on Economic Management and Model Engineering
650

an ophthalmologist at the Central Hospital of Wuhan,
forwarded text messages that 7 cases of SARS were
diagnosed in the South China Fruit and Seafood
Market in the WeChat group, with a photo of clinical
pathogen screening results and a video of lung
examination as a reminder for relatives and friends to
take precautions. As news of the epidemic spread,
Wuhan's work arrangements for the prevention and
control of unexplained pneumonia, by-laws and
regulations on the prevention and control of
infectious diseases, public security management, and
other laws and regulations, as well as the notification
of the Municipal Health Commission, the public
security administration of Wuhan started to
investigate the information on infectious diseases on
the Internet. Investigate the situation. On January 3,
2020, the Zhongnan Road Police Station of the
Wuchang Branch of the Wuhan Public Security
Bureau contacted Doctor Li Wenliang, and then he
and his colleagues came to the police station for a
conversation, and finally, Doctor Li Wenliang was
given a letter of admonition(2020).
After learning about the pneumonia of unknown
cause in Wuhan through other channels, National
Health Commission sent an expert team to Wuhan to
discuss the “pneumonia of unknown cause” with the
staff of the Wuhan Municipal Health Commission on
December 31, 2019. On the same day, Wuhan
Municipal Health Commission released news that 27
cases of pneumonia of unknown cause were found in
Wuhan through its official media platform, and that
“so far no obvious human-to-human transmission has
been found in the investigation, and no medical staff
infection has been found(About the Current Situation
of the City’s COVID-19 Outbreak, 2019)”. Among
the 138 consecutive patients admitted to Zhongnan
Hospital of Wuhan University from January 1st to 28,
the proportion of medical staff was as high as
29%(Wang B X et al., 2020). The Wuhan Municipal
Health and Family Planning Commission issued the
“Manual for Medical Treatment of Unexplained
Viral Pneumonia” on January 4, which stipulates that
for suspected cases, the hospital should organize
expert consultation within 12 hours, and the results of
the diagnosis should be immediately reported online
when there is suspected pneumonia of unknown
cause. Two more adjustments were subsequently
made, as shown in Table 1.
Table 1: Changes in the reporting process of the online direct reporting system.
Time File name
The reporting process of the network direct reporting
system
2006
Administrative Measures for Monitoring
Information Reporting of Public Health
Emergencies and Infectious Disease
Epidemic Situations
The responsible reporting unit or person-make a direct
online report immediately (within 2 hours).
2020.0
1.04
Wuhan Municipal Health Commission
“Work Manual for Medical Treatment of
Unexplaine
d
Viral Pneumonia”
Primary doctors discover suspected cases-relevant
departments organize expert consultation-hospitals/medical
institutions-report directly online (within 12 hours).
2020.0
1.05
Wuhan Municipal Health Commission
“Work Manual for Medical Treatment of
Unexplained Viral Pneumonia”
Primary doctors discover suspected cases-relevant
departments organize expert consultation-hospitals/medical
institutions-district health commissions organize expert
consultation-report directly online.
2020.0
1.10
Wuhan hospitals received oral notices from
relevant staff of municipal and provincial
health commissions
Primary doctors discover suspected cases-relevant
departments organize expert consultations-
hospitals/medical institutions-district health Commission
organizes expert consultation-Municipal Health
Commission organizes expert consultation-Provincial
Health Committee organizes expert consultation-report
directly online.
In the 2006 revised version of the “Administrative
Measures for Monitoring Information Reporting of
Public Health Emergencies and Infectious Disease
Epidemic Situations”, “direct reporting on the
Internet” does not require other levels of review and
consultation, although it also requires the
consultation of county, municipal and provincial
levels. However, the purpose of the consultation is to
“exclude the possibility of SARS”. The consultation
is not a prerequisite for “direct online reporting”, but
to facilitate the revision of the results of previous
online direct reporting and issue early warnings and
Analysis of the Current Situation and Problems of China’s National Infectious Disease Network Direct Reporting System Under the
COVID-19
651

take appropriate preventive and control measures on
time. By contrast, it can be seen that in just a few days
from January 4 to January 10, 2020, the original
reporting method that the cases can be reported
directly online once it is confirmed by the primary
clinician has changed to the way by which direct
online reporting is only possible after expert
consultations organized by the district, city, and
provincial health commissions at all levels, as well as
the approval of the provincial health commission.
Until January 24, when the unknown virus was
officially named “new-coronavirus” (COVID-19)
and the emergency system was debugged, the
“dynamic monitoring function of pneumonia caused
by new coronavirus infection” of the infectious
disease network direct reporting system was finally
launched.
4 CONCLUSION
Undoubtedly it is particularly important to have easy
access to online reporting for infectious diseases, but
at the beginning of the outbreak, due to the
refrainment of reporting authority, the Hubei
Provincial Health Commission kept claiming “no
increase” until January 15, 2020, but the fact is that
the spread of the virus never stopped during this time.
In addition, even the top level of the NCDC has no
executive power or decision-making authority, which
means it is unable to make policy measures to prevent
and control the outbreak. Therefore, although the
NCDC reported the outbreak to the central
government as soon as possible, before the central
leadership approved the decision, members of the
high-level expert group of the NCDC could do
nothing but remind and urge people to reduce
unnecessary outings and gatherings at the press
conference, which also hindered the prevention work
in the early stage of the epidemic.
First of all, the NCDC in China is a technical
institution that provides technical services, and is
responsible for reporting to higher administrative
departments but is not entitled to release information
to the public. Meanwhile, local CDCs are under the
jurisdiction of the local health commissions and the
local governments. The NCDC, which is supposed to
be the “whistle-blower” for major public health
events, is caught in a dilemma between local
hospitals facing cases or suspected cases and the
National Health Commission (NHC), owing to
administrative decision-making authority. The
reporting of infectious diseases through the direct
network reporting system is still an administrative
act, which means that timely reporting is not the key,
but approval by higher authorities is the key, while at
the same time, the Health and Welfare Commission,
which is not directly involved in technical guidance,
holds the power to release information about the
epidemic. Instead of institutionalization and
professionalization, the legal obligation of direct
reporting on the Internet has become administrative.
On the other hand, January 24, 2020, is the
Chinese Lunar New Year. The “two sessions” and the
“Spring Festival” drew the public attention, and the
original professional direct reporting has become a
political issue related to local economic development
and social stability, and the direct online reporting
system has turned into a political tool instead of
technical service. When reporting cases of infectious
diseases, the Health Commission or local
governments had to take into consideration the
factors such as the possible social instability caused
by outbreaks and even the possible negative impact
on personal promotions. Policymakers attempted to
weaken and conceal the severity of the epidemic,
resulting in opaque reporting of early cases of the
epidemic, which did not attract sufficient attention
from higher levels of government and thus failed to
effectively control the outbreak as early as possible.
Besides, a complex and accurate report of infectious
diseases can be finished by a single physician under
a normal situation. However, at the beginning of the
outbreak, all the hospitals in Wuhan received at least
200 to 300 outpatients every day, and the number of
patients with pneumonia of unknown cause increased
rapidly. It was hard for doctors to report online,
which exposed the loopholes of the current online
reporting system.
All in all, the case study of the failure of China’s
infectious disease network direct reporting system
implies that scientific and technological means such
as digital government cannot replace the
government’s scientific management, power
distribution, and balance. Infectious disease
prevention and control work is a complex system
arrangement instead of technical work only. At the
same time, it is quite important to properly broaden
the audience of the monitoring system, facilitate the
operation and open the data. Therefore, it is
recommended to explore the automatic reporting
model of the hospital, which can reduce costs and the
possibility of false reporting and concealment. At the
national level, it is recommended that the NCDC be
directly led by the State Council, or managed by the
National Health Commission on behalf. If it extends
downwards, it is possible to merge the local NCDC
and the disease control department of the Health
ICEMME 2022 - The International Conference on Economic Management and Model Engineering
652

Commission. At present, the two sectors overlap in
some work at the grassroots level, which is not
helpful for prevention and control in a state of crisis.
REFERENCES
About the current situation of the city's COVID-19
outbreak. (2019, December 31). Wuhan Municipal
Health Committee.
http://wjw.wuhan.gov.cn/gsgg/202004/t20200430_11
99576.shtml
Development of health and progress of human rights in
China. (2017). The State Council Information Office of
the People's Republic of China.
http://www.scio.gov.cn/zfbps/ndhf/36088/Document/1
565111/1565111.htm
Huang X S, Qiu Y H, Wu Y S, & Lan Y P. (2008).
Problems of Direct Reporting of Infectious Diseases in
Hospitals and Countermeasures. China Journal of
Misdiagnosis, 34, 8413–8414.
Li M, & Zhang Z. (2011). Problems of the current direct
reporting system for infectious diseases and
countermeasures. Jiangsu Health Affairs Industry
Management, 22(05), 111–113.
Ma J Q, Yang G H, & Shi X M. (2006). IT-based
technology platform for disease surveillance in China.
Disease Surveillance, 01, 1–3.
Report on the investigation of the situation involving Dr. Li
Wenliang. (2020, March 20). Central Discipline
Inspection Commission State Supervision Commission
website.
https://www.ccdi.gov.cn/toutiaon/202003/t20200319_
97107.html
Wang G H. (1996). China Infectious Disease Surveillance
Reporting System. Management Information System,
02, 16–18.
Wang B X, Yuan Y T, Zhang L, Zhang Z Z, & Fu L G.
(2020). Trend of novel coronavirus pneumonia death
cases and their characteristics from onset to time of
death. Journal of Bengbu Medical College, 45(02),
141–147. https://doi.org/10.13898/j.cnki.issn.1000-
2200.2020.02.001
Why did the direct network reporting system fail in Wuhan
at the beginning of the epidemic? (2020, March 15).
PengPai News.
https://www.thepaper.cn/newsDetail_forward_652397
4
Xu W, & Chen S. (2020, February 4). The outbreak
reporting system behind the COVID-19. BJNEWS.
http://www.bjnews.com.cn/news/2020/02/04/684397.
html
Analysis of the Current Situation and Problems of China’s National Infectious Disease Network Direct Reporting System Under the
COVID-19
653
